Articles
- Page Path
- HOME > J Trauma Inj > Volume 37(1); 2024 > Article
-
Original Article
Chest wall injury fracture patterns are associated with different mechanisms of injury: a retrospective review study in the United States -
Jennifer M. Brewer, MD1
 , Owen P. Karsmarski, BS1, Jeremy Fridling, MD1, T. Russell Hill, BS2, Chasen J. Greig, MD2, Sarah E. Posillico, MD2, Carol McGuiness, BS2, Erin McLaughlin, BS2, Stephanie C. Montgomery, MD2, Manuel Moutinho, MD2, Ronald Gross, MD2, Evert A. Eriksson, MD3, Andrew R. Doben, MD2
, Owen P. Karsmarski, BS1, Jeremy Fridling, MD1, T. Russell Hill, BS2, Chasen J. Greig, MD2, Sarah E. Posillico, MD2, Carol McGuiness, BS2, Erin McLaughlin, BS2, Stephanie C. Montgomery, MD2, Manuel Moutinho, MD2, Ronald Gross, MD2, Evert A. Eriksson, MD3, Andrew R. Doben, MD2 -
Journal of Trauma and Injury 2024;37(1):48-59.
DOI: https://doi.org/10.20408/jti.2023.0065
Published online: February 23, 2024
- 624 Views
- 16 Download
1Department of General Surgery, University of Connecticut School of Medicine, Farmington, CT, USA
2Department of Surgery, Saint Francis Hospital and Medical Center, Hartford, CT, USA
3Department of Surgery, Medial University of South Carolina, Charleston, SC, USA
- Correspondence to Jennifer M. Brewer, MD Department of General Surgery, University of Connecticut School of Medicine, 200 Academic Wy, Farmington, CT 06032, USA Tel: +1-860-679-2000 Email: jenbrewer830@gmail.com
© 2024 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Purpose
- Research on rib fracture management has exponentially increased. Predicting fracture patterns based on the mechanism of injury (MOI) and other possible correlations may improve resource allocation and injury prevention strategies. The Chest Injury International Database (CIID) is the largest prospective repository of the operative and nonoperative management of patients with severe chest wall trauma. The purpose of this study was to determine whether the MOI is associated with the resulting rib fracture patterns. We hypothesized that specific MOIs would be associated with distinct rib fracture patterns.
-
Methods
- The CIID was queried to analyze fracture patterns based on the MOI. Patients were stratified by MOI: falls, motor vehicle collisions (MVCs), motorcycle collisions (MCCs), automobile-pedestrian collisions, and bicycle collisions. Fracture locations, associated injuries, and patient-specific variables were recorded. Heat maps were created to display the fracture incidence by rib location.
-
Results
- The study cohort consisted of 1,121 patients with a median RibScore of 2 (range, 0–3) and 9,353 fractures. The average age was 57±20 years, and 64% of patients were male. By MOI, the number of patients and fractures were as follows: falls (474 patients, 3,360 fractures), MVCs (353 patients, 3,268 fractures), MCCs (165 patients, 1,505 fractures), automobile-pedestrian collisions (70 patients, 713 fractures), and bicycle collisions (59 patients, 507 fractures). The most commonly injured rib was the sixth rib, and the most common fracture location was lateral. Statistically significant differences in the location and patterns of fractures were identified comparing each MOI, except for MCCs versus bicycle collisions.
-
Conclusions
- Different mechanisms of injury result in distinct rib fracture patterns. These different patterns should be considered in the workup and management of patients with thoracic injuries. Given these significant differences, future studies should account for both fracture location and the MOI to better define what populations benefit from surgical versus nonoperative management.
- Background
- Rib fractures remain among the most common injuries after blunt trauma. They are documented in approximately 40% of all blunt trauma cases and they are a significant cause of morbidity and mortality associated with blunt force trauma [1–3]. Increasing morbidity and poor outcomes are generally associated with older age and a greater number and extent of fractures [4–6]. Rib fractures are generally diagnosed during the initial trauma workup, utilizing chest x-rays and computed tomography (CT). Even with modern computerized reconstructions, however, up to 30% of rib fractures are missed on initial imaging [7,8]. Significant concomitant injuries, such as traumatic diaphragmatic injury, can also be missed on CT [1]. The mechanism of injury (MOI) is an important predictor of the extent of injury in trauma patients [9–11]. Incorporating the MOI early in the triage process leads to better outcomes [9,10].
- Once rib fractures are diagnosed, morbidity can be reduced by promptly initiating the appropriate treatment. Multidisciplinary clinical pathways have been utilized to reduce ventilator-dependent days, length of stay, infectious morbidity, and mortality [6,12], and high-volume institutions have created chest wall injury and reconstructive centers to improve patient outcomes [13]. However, a proper diagnosis can be challenging, even with current CT technology. The limits of current technology can lead to delays in diagnosis and thus treatment. If the injury pattern and severity could be anticipated based on the MOI, fewer injuries would be missed, and earlier intervention likely would improve patient care. The MOI could be added to rib fracture protocols, aiding in the identification of patients appropriate for nonoperative management, locoregional anesthesia, or early surgical stabilization of rib fractures (SSRF), where improved outcomes have been shown with earlier fixation [14].
- Objectives
- The purpose of this study was to analyze fracture patterns based on different MOIs, including falls, motor vehicle collisions (MVCs), motorcycle collisions (MCCs), automobile striking a pedestrian (automobile-pedestrian collisions), and bicycle collisions. This study investigated whether the fracture location was associated with the MOI. We hypothesized that specific MOIs would be associated with distinct fracture patterns. This information will provide further insight into anticipating patient needs for other associated injuries, treatment pathways, critical care, and disposition.
INTRODUCTION
- Ethics statement
- This study was approved by the Institutional Review Board of St. Francis Medical Center (No. 22-47). Informed consent was waived due to the retrospective nature of the study.
- Study design and setting
- We performed a retrospective analysis of de-identified, prospectively collected data contained within the Chest Injury International Database (CIID), an international database of the Chest Wall Injury Society (CWIS). The CIID is a Health Insurance Portability and Accountability Act (HIPAA)-compliant, cloud-based data repository for the members of the CWIS to support international research collaboration. The CIID contains over 100 standardized datapoints per patient, with a granular dataset including fracture patterns and chest injury–specific outcomes (Table 1). CIID contains both operative and nonoperative patients. The data are volunteered from CWIS-member institutions and entered by verified individuals at each site. The criteria for entering a patient are specific to each site, with some institutions entering all patients with rib fractures, while others enter only patients who undergo SSRF. There is no cost for the contribution or data collaboration for centers that participate in CIID.
- Patients
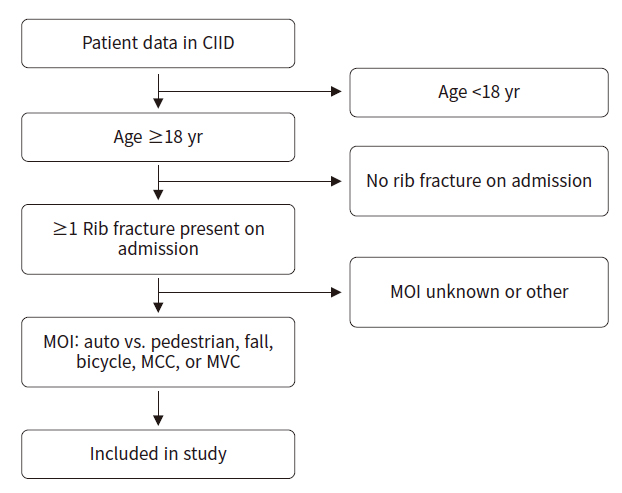
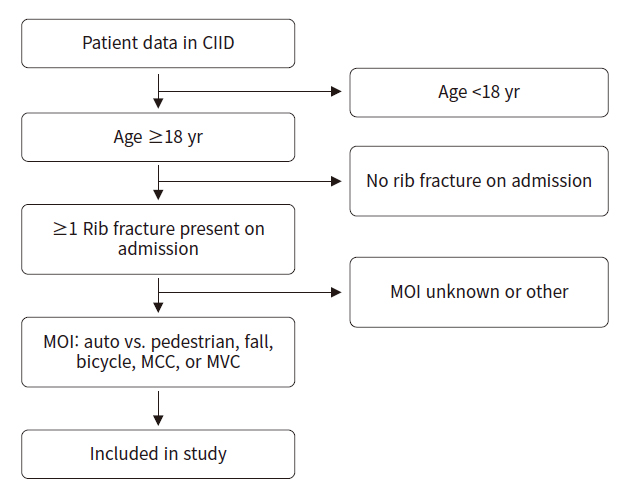
- We included all patients over the age of 18 with rib fractures who were admitted to the hospital. We excluded any patient less than 18 years old. Trauma MOIs were categorized as automobile-pedestrian collisions, falls, bicycle collisions, MCCs, or MVCs (Fig. 1).
- We did not include patients with missing data in the analysis. At the time of data extraction, there were 1,601 patients in the database. Only 1,121 had a complete dataset for this analysis. The patients with missing data were from data imports of individual data registries from different centers. These patients’ data were imported but did not contain all the data points of the CIID; therefore the data were excluded from the analysis dataset. For the 1,121 patients included in the study, there were no missing data points in the variables analyzed. Matching was not necessary since a complete dataset was analyzed, and the authors did not want to create data for the missing variables.
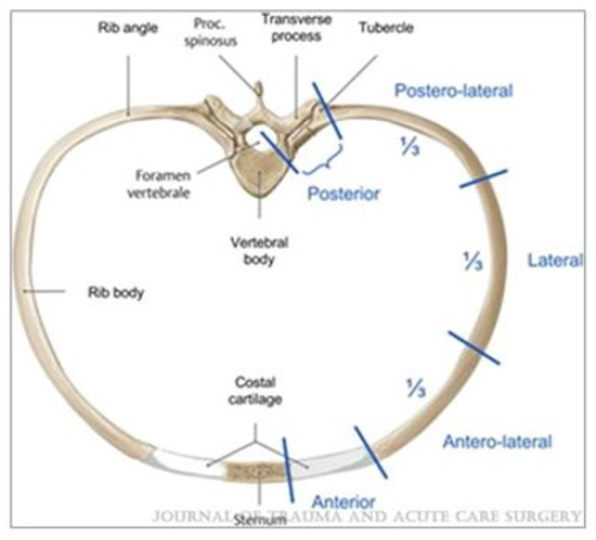
- The extracted data consisted of fracture patterns based on MOI, and the locations of fractures as defined by CWIS nomenclature [15]. This includes the following: anterior, anterolateral, lateral, posterolateral, and posterior (Fig. 2) [16]. Further extracted data are presented in Table 1.
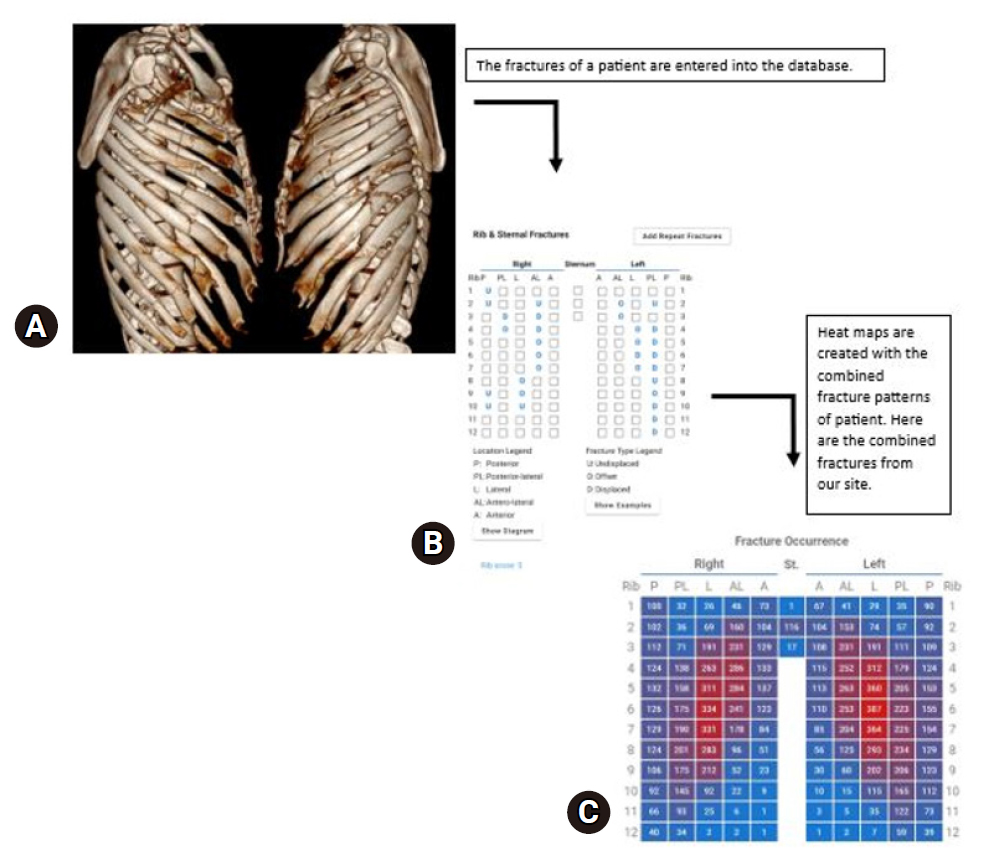
- Heat maps were generated to display the location of the fractures and the individual number of fractures in each location. Heat map explanations are provided in Fig. 3. The data were stratified based on MOI. Our primary endpoint was to assess chest wall injuries and match the clinical injury to the mechanism based on observed distribution patterns. The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guideline was used to ensure proper reporting of the methods, results, and discussion.
- Statistical analysis
- Statistical analysis comparing the MOI and patterns of rib fracture injury was carried out with IBM SPSS ver. 26.0 (IBM Corp). Continuous variables were assessed with the Student t-test when normally distributed and the Wilcoxon signed rank sum test when skewed. The Mann-Whitney U-test was used to assess rank sums of data without a normal distribution. We defined statistical significance as a P-value of ≤0.05 in all statistical analyses. We did not include missing data in the analysis.
METHODS
- Demographic data
- The study population was 64% male, with an average age of 57 years (Table 2). The median RibScore was 2 (range, 0–3) and there were 9,353 individual fractures noted in 1,121 patients.
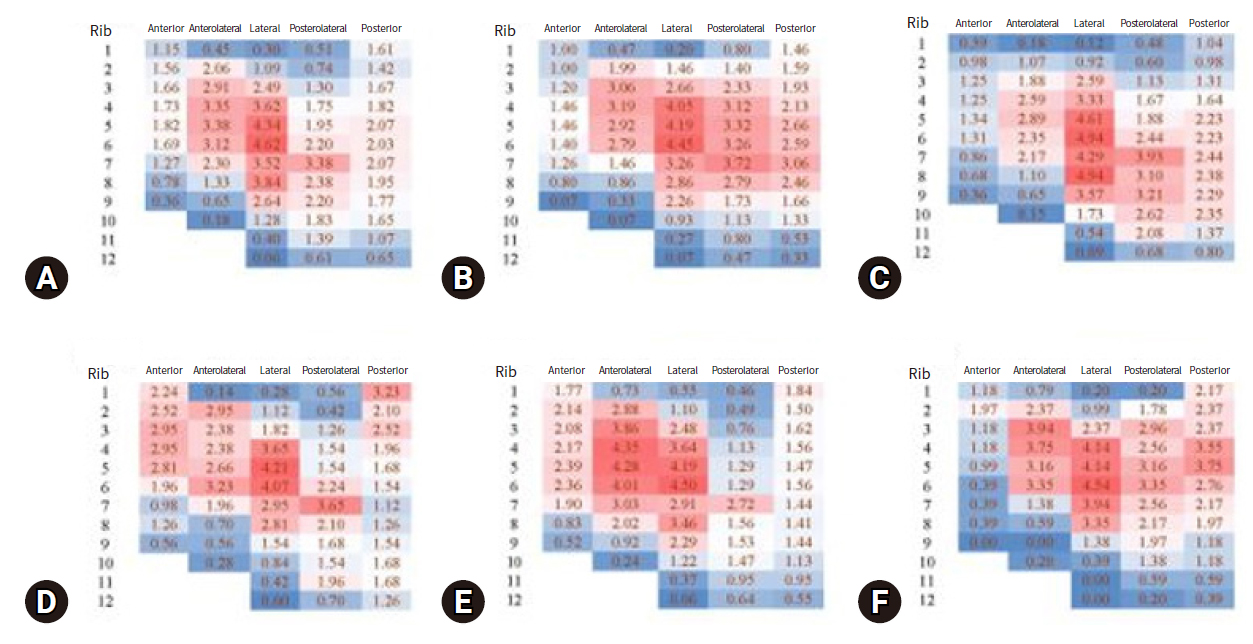
- The most significant results of the study are shown in the heatmaps comparing the MOI and rib fracture injury patterns (Figs. 4, 5). Overall, based on the study results, the fifth and sixth ribs were fractured the most at the lateral portion of the rib with frequencies of 4.34 and 4.56, respectively. The lowest number of fractures was recorded for lateral rib fractures in the first and twelfth ribs, with frequencies of 0.30 and 0.06, respectively. MCCs showed a pattern with the highest fracture rate in the lateral position of the fifth and sixth ribs, with frequencies of 4.19 and 4.45, respectively. Falls demonstrated a pattern where the highest fracture rate was in the lateral positions of the sixth and eighth ribs, with frequencies of 4.94 and 4.94, respectively. Automobile-pedestrian collisions showed a pattern with the highest fracture rate in the lateral positions of the fifth and sixth ribs, with frequencies of 4.21 and 4.07, respectively. On average, MVCs and MCCs had nine fractures per patient, while bicycle collisions had 8.5, automobile-pedestrian collisions had 10, and falls had seven fractures per patient. MVCs demonstrated a pattern with the highest fracture rate in the lateral position of the sixth rib and in the anterolateral position of the fourth rib, with frequencies of 4.50 and 4.35, respectively. Lastly, bicycle collisions demonstrated a pattern where the highest fracture rate was in the lateral positions of the fourth and sixth ribs, with frequencies of 4.14 and 4.54, respectively (Fig. 4).
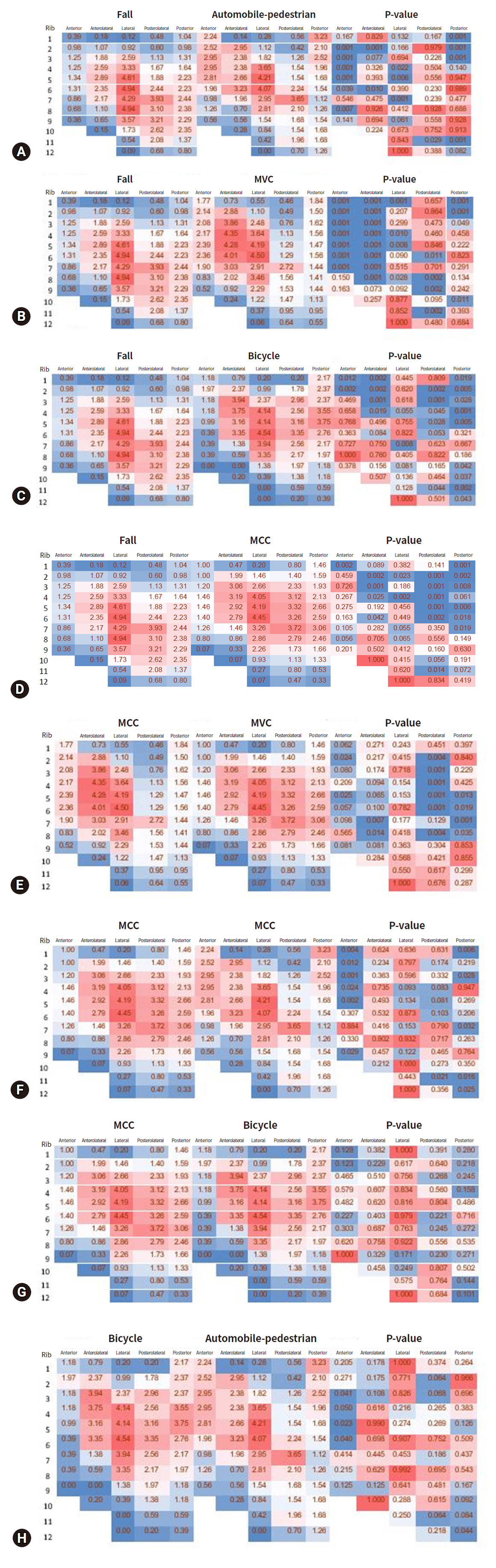
- Comparisons of each MOI were made. For statistical purposes, falls were set as the standard for comparison, as this tends to be the most common recent MOI in trauma centers. When comparing falls versus automobile-pedestrian collisions, statistically significant differences were seen for anterior second to sixth and eighth ribs and posterior first to third ribs. When comparing falls versus bicycles, significant differences were seen for anterior first and second ribs, anterolateral first to third ribs, posterolateral second to fifth ribs, posterior first to fifth ribs, and posterior ninth to twelfth ribs. When comparing falls versus MCCs, significant differences were seen for posterolateral second to sixth ribs, posterolateral eleventh rib, and posterior first to seventh ribs. When comparing falls versus MVC, significant differences were seen for anterior first to seventh ribs and anterolateral first to eighth ribs (Fig. 5).
- We then sought to compare separate mechanisms. When comparing MVCs versus MCCs, significant differences were seen with anterior second and fifth ribs and posterolateral second to sixth ribs. When comparing MCCs versus bicycles, no statistically significant differences were observed between these two groups. When comparing bicycle versus automobile-pedestrian collisions, significant differences were seen for anterior third to sixth ribs (Fig. 5).
RESULTS
- There is little information linking the MOI with rib fracture patterns, specifically at the level of detail that is captured within CIID. We sought to investigate whether certain MOIs correlate with certain fracture patterns so that we may specifically target imaging, accelerate diagnosis, and more carefully identify other surrounding at-risk structures based on the fracture pattern. It is well documented in the literature that CT scans miss rib fractures [14,15,17,18]. It is also well documented in the literature that rib fractures are associated with other injuries, but we do not know if the MOI is associated with rib fractures and other injury patterns [19–20]. If a specific injury pattern could be predicted based on the MOI, focused imaging modalities such as three-dimensional (3D) rendering and use of arterial phase CT scans could be tailored to the correct mechanism. In patients too unstable for imaging who proceed directly to the operating room, the MOI could be used to predict rib fractures and injuries to nearby structures in the neck, chest, or abdomen. These predictions potentially could guide operative decision-making when time is critical.
- The major finding of this investigation is that there is a significant association between the MOI and rib fracture pattern. This is demonstrated by the statistically significant differences among the different MOIs and rib fracture patterns in the associated locations. To our knowledge this is the first such investigation evaluating the MOI and fracture patterns in living patients [16,17,21]. Lateral rib fractures were, as expected, the most common location for fractured ribs. MVCs showed a trend toward anterior, while falls trended toward posterior rib fractures (Fig. 4). Clinically, this makes sense, as high-impact MVCs involve passive and active restraint devices and usually a frontal impact, while patients who fall often land on their backs or tucked arms.
- We also hypothesize that mechanisms with similar levels of energy seem to be associated with similar injury patterns. MVCs and MCCs on average had nine fractures per patient, while bicycle collisions had 8.5, automobile-pedestrian collisions had 10, and falls had seven fractures per patient; thus, falls exhibited fewer similarities in rib fracture patterns compared to automobile-pedestrian collisions, MCCs, and MVCs and on average had fewer ribs fractured (Fig. 4). MVCs and MCCs had statistical differences in the posterolateral location (Fig. 4). This could be largely due to the mechanism of impact, considering both are higher velocity impacts. These novel findings will enable radiologists and surgeons to target their radiologic workup more specifically, as to identify rib fractures and associated injuries more quickly and with greater reliability. In turn, we hope this will allow providers to act more promptly in the care of patients with blunt force trauma and suspected rib injuries. For instance, a patient presenting after MCC can be examined more closely physically and via imaging, looking for posterior rib fractures and concomitant injuries to the aorta.
- Our data are congruent with the limited literature available, and this study’s advantages include a greater sample size, a standard taxonomy, and more precise information by utilizing the CIID [4,22]. The CIID uses the published CWIS taxonomy for fractures, which the authors hope will be incorporated in all future studies to provide standardization, specificity, and scalability to future findings.
- We report here a novel study describing an association between the MOI and specific rib fracture patterns. These results suggest that one may be able to predict the rib fracture pattern based on the MOI. This may assist providers to specifically look for these predicted fracture patterns with appropriate and focused radiographic studies, thereby allowing for fewer missed injuries and earlier, appropriate intervention (s). This ability to arrive more rapidly at accurate diagnoses could lead to improved outcomes for patients who experience thoracic trauma with significant rib fractures and associated injuries.
- Linking the MOI and rib fracture injury patterns may help us detect various injuries, one in particular has much promise: diaphragm injuries. Lower rib fractures are already associated with diaphragm injuries. Specific studies have linked low-grade liver or spleen injuries with rib fractures to a 20% rate of diaphragm injury [23]. Another group [24] performed thoracoscopy to reveal diaphragm injuries during SSRF; they found a rate of 16.5%. Even when a radiologist reviewed these CT scans, 77% of the diaphragm injuries were missed. Being able to link the MOI with rib fracture injuries to diaphragmatic injuries may lead us to a new algorithm for performing diagnostic laparoscopy in certain patients.
- Even if these missed rib fractures on CT scans are not clinically relevant, patients want to know all their injuries for personal and litigation purposes. If we know we are missing rib fractures on CT scans based on certain mechanisms, 3D reconstructive images may be ordered. At certain high-volume centers, 3D reconstructive images are obtained for all rib fracture patients, but this could be a waste of resources; knowing what MOI is associated with certain rib fracture patterns could help us to be more selective when deciding who gets 3D reconstructive images.
- Limitations
- Our study is most significantly limited by its sample population of 1,121 patients, primarily from chest wall centers, which may introduce a selection bias. The population is further limited by variable database-entry criteria at each institution, with some institutions entering all patients with rib fractures, and others only entering patients who undergo SSRF. Patients are only entered by chest wall surgeons, meaning the less-injured patient that does not require a surgical consult would not be submitted into the registry. As the CIID grows, more sites will be recruited to utilize the database, and CWIS hopes to standardize the criteria for populating the database across participating institutions. Another limitation of the study is the inclusion and exclusion criteria, as there may be other variables that influence rib fracture pattern and location that were not accounted for in this study. One in particular is age. Due to fragility, older patients more easily break ribs. Future studies should assess whether the MOI, age, and rib fracture injury patterns are related. In the future, we can use matched cohorts to control for this potential confounder.
- Conclusions
- Unique rib fracture patterns are generated by different mechanisms of injury. These patterns should be considered when conducting evaluations, assessing the possible use of diagnostic modalities, and considering the need for potential interventions on patients with acute thoracic trauma. Future studies should evaluate additional variables such as age, the Blunt Pulmonary Contusion 18 (BPC18) score factor, and SSRF and their association with MOI and fracture pattern. Research focusing on the association between MOI and rib fracture patterns, and the implications of morbidity and mortality, is ongoing.
DISCUSSION
-
Author contributions
Conceptualization: JMB, OPK; Data curation: ARD; Formal analysis: JMB, EAE, ARD; Methodology: JMB, OPK; Project administration: JMB; Visualization: JMB; Writing–original draft: all authors; Writing–review & editing: all authors. All authors read and approved the final manuscript.
-
Conflicts of interest
Evert A. Eriksson is an educational speaker for DePuy Synthes. Andrew R. Doben received royalties for an unrelated product from Zimmer Biomet and is an educational consultant for KLS Martin. The authors have no other conflicts of interest to declare.
-
Funding
The authors received no financial support for this study.
-
Data availability
Data analyzed in this study are available from the corresponding author upon reasonable request.
ARTICLE INFORMATION
- 1. Caragounis EC, Xiao Y, Granhed H. Mechanism of injury, injury patterns and associated injuries in patients operated for chest wall trauma. Eur J Trauma Emerg Surg 2021;47:929–38. ArticlePubMedPMCPDF
- 2. Bulger EM, Arneson MA, Mock CN, Jurkovich GJ. Rib fractures in the elderly. J Trauma 2000;48:1040–7. ArticlePubMed
- 3. Brasel KJ, Moore EE, Albrecht RA, et al. Western Trauma Association critical decisions in trauma: management of rib fractures. J Trauma Acute Care Surg 2017;82:200–3. PubMed
- 4. Sirmali M, Turut H, Topcu S, et al. A comprehensive analysis of traumatic rib fractures: morbidity, mortality and management. Eur J Cardiothorac Surg 2003;24:133–8. ArticlePubMed
- 5. Shulzhenko NO, Zens TJ, Beems MV, et al. Number of rib fractures thresholds independently predict worse outcomes in older patients with blunt trauma. Surgery 2017;161:1083–9. ArticlePubMed
- 6. Todd SR, McNally MM, Holcomb JB, et al. A multidisciplinary clinical pathway decreases rib fracture-associated infectious morbidity and mortality in high-risk trauma patients. Am J Surg 2006;192:806–11. ArticlePubMed
- 7. Lerner EB, Badawy M, Cushman JT, et al. Does mechanism of injury predict trauma center need for children? Prehosp Emerg Care 2021;25:95–102. ArticlePubMedPMC
- 8. Lupton JR, Davis-O’Reilly C, Jungbauer RM, et al. Mechanism of injury and special considerations as predictive of serious injury: a systematic review. Acad Emerg Med 2022;29:1106–17. ArticlePubMedPMCPDF
- 9. Kissling S, Hausmann R. Morphology of direct and indirect rib fractures. Int J Legal Med 2021;135:213–22. ArticlePubMedPDF
- 10. Macheel C, Reicks P, Sybrant C, et al. Clinical decision support intervention for rib fracture treatment. J Am Coll Surg 2020;231:249–56. ArticlePubMedPMC
- 11. Brewer JM, Huselid R, Petitpas KM, et al. Creating a Chest Wall Injury and Reconstructive program: a single center experience with rib fractures. Injury 2022;53:4013–9. ArticlePubMed
- 12. Prins JT, Wijffels MM, Pieracci FM. What is the optimal timing to perform surgical stabilization of rib fractures? J Thorac Dis 2021;13(Suppl 1):S13–25. ArticlePubMedPMC
- 13. Edwards JG, Clarke P, Pieracci FM, et al. Taxonomy of multiple rib fractures: results of the chest wall injury society international consensus survey. J Trauma Acute Care Surg 2020;88:e40–5. ArticlePubMed
- 14. Cho SH, Sung YM, Kim MS. Missed rib fractures on evaluation of initial chest CT for trauma patients: pattern analysis and diagnostic value of coronal multiplanar reconstruction images with multidetector row CT. Br J Radiol 2012;85:e845–50. ArticlePubMedPMC
- 15. Sirlin CB, Brown MA, Deutsch R, et al. Screening US for blunt abdominal trauma: objective predictors of false-negative findings and missed injuries. Radiology 2003;229:766–74. ArticlePubMed
- 16. Sarani B, Allen R, Pieracci FM, et al. Characteristics of hardware failure in patients undergoing surgical stabilization of rib fractures: a Chest Wall Injury Society multicenter study. J Trauma Acute Care Surg 2019;87:1277–81. ArticlePubMed
- 17. Hu J, Zheng ZF, Wang SH, Si DL, Yuan YQ, Gao BL. Missed rib fractures on initial chest CT in trauma patients: time patterns, clinical and forensic significance. Eur Radiol 2021;31:2332–9. ArticlePubMedPDF
- 18. Liu C, Chen Z, Xu J, Wu G. Diagnostic value and limitations of CT in detecting rib fractures and analysis of missed rib fractures: a study based on early CT and follow-up CT as the reference standard. Clin Radiol 2022;77:283–90. ArticlePubMed
- 19. Davoodabadi A, Mosavibioki N, Mashayekhil M, Gilasi H, Kashi EA, Haghpanah B. Correlation of rib fracture patterns with abdominal solid organ injury: a retrospective observational cohort study. Chin J Traumatol 2022;25:45–8. ArticlePubMedPMC
- 20. Lee EL, Craig M, Scarboro M. Real-world rib fracture patterns in frontal crashes in different restraint conditions. Traffic Inj Prev 2015;16 Suppl 2:S115–23. ArticlePubMed
- 21. Scheirs S, Langenhorst W, Malgosa A, et al. Perimortem fracture pattern in ribs by blunt force trauma. Int J Legal Med 2018;132:1205–13. ArticlePubMedPDF
- 22. Chien CY, Chen YH, Han ST, Blaney GN, Huang TS, Chen KF. The number of displaced rib fractures is more predictive for complications in chest trauma patients. Scand J Trauma Resusc Emerg Med 2017;25:19. ArticlePubMedPMCPDF
- 23. Plurad DS, Nielsen JS, Hancock J, et al. Concomitant rib fractures and minor liver or spleen injuries in blunt trauma: what is the potential for missed diaphragmatic injuries? Am Surg 2010;76:380–4. ArticlePubMedPDF
- 24. Wemeijer TM, Hogeboom W, Steenvoorde P, Withaar DS, de Groot R. Missed injuries in trauma patients: the value of a diagnostic thoracotomy or thoracoscopy during surgical stabilisation of rib fractures. Ir J Med Sci 2022;191:1285–9. ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite