Comparison of Outcomes and Recurrence in Chronic Subdural Hematoma Patients Treated by Burr-Hole Drainage with or without Irrigation
Article information
Abstract
Purpose
Chronic subdural hematoma (CSDH) is a common disease in elderly patients and is usually treated by burr-hole drainage. However, the optimal surgical technique for treating CSDH has not been determined. In this study, we analyzed outcomes and recurrence rates after burr-hole drainage with or without irrigation in patients with CSDH.
Methods
Eighty-two CSDH patients treated with burr-hole drainage at Wonju Severance Christian Hospital from March 2015 to June 2016 were enrolled in this study. The subjects were divided into three groups based on the surgical technique performed as follows: single burr-hole drainage without irrigation (group A, n=47), single burr-hole drainage with irrigation (group B, n=14), or double burr-hole drainage with irrigation (group C, n=21). These three groups were compared with respect to clinical and radiological factors and the recurrence rate, and independent factors predicting recurrence were sought.
Results
After burr-hole drainage, CSDH recurred in 15 (18.3%) of the 82 patients, and six patients (7.3%) required reoperation. More specifically, recurrence was observed in 12 patients (25.5%) in group A, one (7.1%) in group B, and two (9.5%) in group C. The number of burr-holes did not significantly affect recurrence (odds ratio [OR]=0.38; 95% confidence interval [CI]: 0.60–2.38), but irrigation had a significant effect (OR=0.20; 95% CI: 0.04–0.97).
Conclusions
This study shows that irrigation during burr-hole surgery in CSDH patients significantly reduced the risk of recurrence, regardless of the number of burrholes used. We therefore recommend the use of active irrigation during burr-hole drainage surgery in CSDH patients.
INTRODUCTION
Chronic subdural hematoma (CSDH) is a relatively common neurosurgical disease, especially in elderly patients [1-5]. In 2016, its global incidence was reported to be 1–13.5 per 100,000 per year [2], and its incidence continues to increase concomitantly with population aging [4,6]. In roughly two-thirds of cases (most commonly in men), there is a history of minor trauma [2]. Although small CSDHs can be resolved without surgery, surgical treatment is required in most cases [2]. The prognosis of CSDH is relatively favorable, but the postoperative recurrence rate has been reported to range widely, from as little as 2% to as high as 37% [1,2,5,7-10].
Single burr-hole craniostomy and drainage is the most commonly used treatment modality [1,5,8,11], but various surgical techniques, such as multi burr-hole craniostomy, massive irrigation, irrigation with thrombin, small or large craniotomy, and membranectomy, have been reported to reduce recurrence [1,2,11-17], and as a result, controversy exists regarding the optimal surgical method for CSDH.
The present study was performed to compare CSDH recurrence rates after single or double burr-hole drainage with or without irrigation, with the ultimate aim of determining which method is most effective for reducing recurrence.
METHODS
Patient selection
We retrospectively studied the archived medical records of patients who underwent burr-hole craniostomy with drainage for CSDH at a single institution from March 2015 to June 2016. Surgical procedures were classified into the following three groups according to the surgical procedure used at the surgeon’s discretion: single burr-hole craniostomy with drainage, but without irrigation (group A, n=47); single burr-hole craniostomy with drainage and irrigation (group B, n=14); and double burr-hole craniostomy with drainage and irrigation (group C, n=21). In group C, two large burr-holes were used with massive irrigation through each hole to provide more effective subdural space irrigation. Group selection bias was checked using analysis of variance (ANOVA) or the chi-square test. During the follow-up period, non-recurrence was defined as the absence of new neurological symptoms with no increase in hemorrhage on follow-up brain computed tomography (CT). We excluded one case of craniotomy performed due to postoperative bleeding and another case in which surgery was required for post-craniostomy empyema. The study was approved beforehand by the Institutional Review Board of Yonsei University Wonju College of Medicine (CR317094).
Surgical procedures and management
All patients underwent single or double burr-hole trephination operations with closed drainage under general anesthesia. After dural incision and hemostasis, the outer membrane enclosing the hematoma was opened. In group A, only a drainage catheter was inserted into the hematoma cavity and the operation was terminated. In group B, a drainage catheter was inserted and irrigation was performed through the catheter. In group C, irrigation was performed directly through two burr-holes, so that the irrigation fluid flowing through one burr-hole came out through the other burr-hole, and after sufficient irrigation, a drainage catheter was inserted into the subdural space. In principle, in all patients who received irrigation, it was performed with cold normal saline until the color of the drainage fluid became clear. After surgery, the drainage catheter was connected to a closed drainage system, and all patients were maintained in the supine position and supplied with sufficient fluid to promote brain expansion. All patients underwent brain CT 3 days after surgery to confirm CSDH reduction, and subsequently at 1-week intervals to check for recurrence. All patients were evaluated for recurrence through at least 10 days of inpatient treatment and at follow-up visits extending for at least 3 months.
Statistical analysis
Data were collected on demographic characteristics, comorbidities, radiological factors, the surgical method, and recurrence. The associations of all variables with recurrence were evaluated using the two-sample t-test or the chi-square test (Fisher’s exact test). Logistic regression analysis was used to identify the degree to which the surgical method could predict CSDH recurrence, and the results were expressed as odds ratio (ORs) with 95% confidence intervals (CIs). Statistical significance was accepted for p-values <0.05, and the analysis was conducted using SPSS version 24.0 (IBM Corp., Armonk, NY, USA).
RESULTS
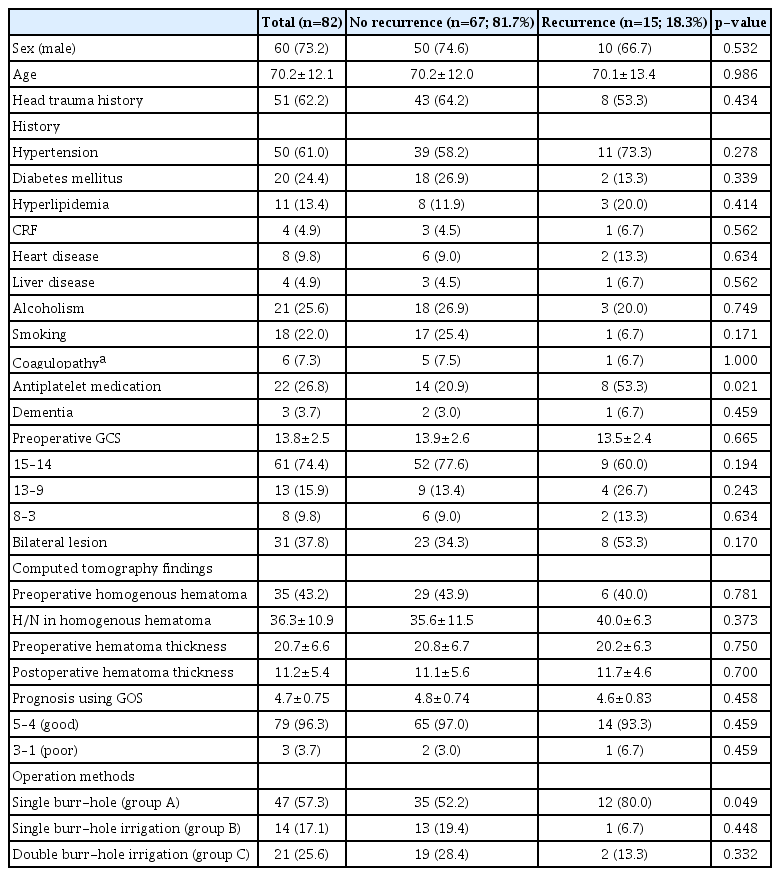
Eighty-two CSDH patients were successfully treated by burr-hole drainage, of whom 73.2% were men. Their mean age was 70.2 years, the overall recurrence rate was 18.3%, and reoperation was required in 7.3% of cases (Table 1).
Patients’ characteristics according to recurrence
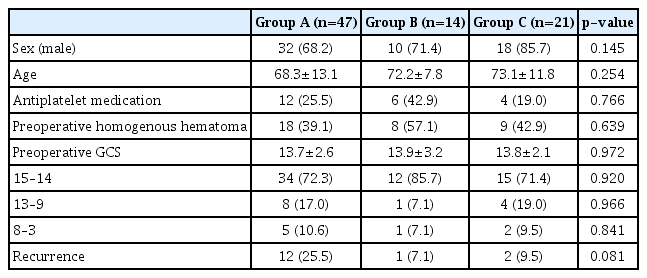
These measures were compared across the three surgical methods using ANOVA for age and the chi-square test for other parameters to justify combining the three groups of patients (Table 2). No significant differences were found among the three surgical methods. Although no significant difference in recurrence was observed among the three study groups, the recurrence rate in group A (single burr-hole craniostomy with drainage, but without irrigation; n=12; 25.5%) was notably higher than that in groups B (n=1; 7.1%) or C (n=2; 9.5%).
Comparison of three surgical methods
Of the demographic factors and preoperative conditions that were analyzed–including patients’ history–only preoperative antiplatelet medication use was found to be significantly related with CSDH recurrence (p=0.021). Furthermore, single burr-hole craniostomy with drainage, but without irrigation, was found to have a significant association with CSDH recurrence (p=0.049) (Table 1).
The number of burr-holes did not significantly affect recurrence (p=0.332) (Table 3). However, the use of intraoperative irrigation was found to reduce the incidence of recurrence (group A vs. groups B and C; p=0.049) (Table 4). Additionally, logistic regression analysis showed that intraoperative irrigation resulted in a statistically significant decrease in the CSDH recurrence rate (OR=0.20; 95% CI: 0.04–0.97), but the use of two burr-holes showed no statistical significance (OR=0.38; 95% CI: 0.60–2.38) (Table 5).
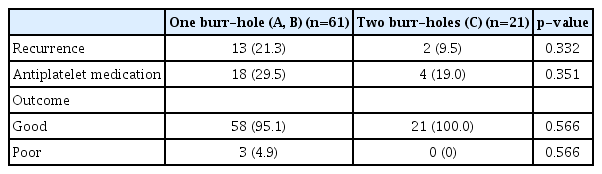
Postoperative outcomes according to the number of burr-holes
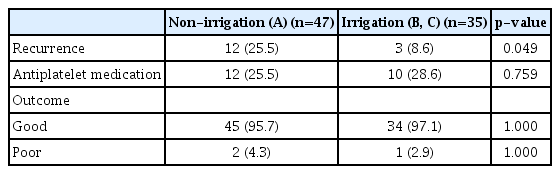
Postoperative outcomes according to intraoperative irrigation status

Logistic regression to calculate ORs for CSDH recurrence after burr-hole operation according to the surgical method used.
DISCUSSION
CSDH is a relatively common disease that usually occurs after mild trauma in the elderly [1,3,8,18]. It is usually treated surgically and has low postoperative morbidity and mortality rates. However, its postoperative recurrence rate is high; therefore, the question of how best to treat CSDH remains a meaningful topic in the neurosurgical field [5,19].
Many studies have investigated CSDH recurrence. The factors reported to be associated with its recurrence after surgery include diabetes, anticoagulant therapy, lack of use of angiotensin-converting enzyme inhibitors, male sex, the presence of bilateral hematomas, a midline shift of ≥1 cm, and presentation with hemiparesis, but the published results contain considerable variation [2,4,12,20-24]. In the present study, the only non-surgical factor found to be associated with recurrence was preoperative antiplatelet medication use.
CSDH is associated with high levels of vasoactive cytokines, inflammatory mediators, and fibrinolytic factors [8,13,25]. Saito et al. [26] reported that the risk of CSDH recurrence increased when high concentrations of these substances remained after surgery, implying that complete evacuation of hematoma during surgery is important. We expected that double burr-hole craniostomy with drainage catheter insertion after massive saline irrigation would remove residual cytokines and fibrinolytic factors more effectively than single burr-hole irrigation and thereby reduce the recurrence rate of CSDH.
The current treatment of choice for CSDH is burr-hole drainage [8], but the optimal surgical technique remains controversial [4]. Taussky et al. [13] reported a higher recurrence rate in a 34-case single burr-hole group than in a group containing 63 cases where two burr-holes were used, but Han et al. [27] reported a higher recurrence rate in a 129-case double burr-hole group than in a 51-case single burr-hole group. In addition, three relatively large retrospective studies reported no significant difference in the recurrence rate between single and double burr-hole procedures [2,28,29], which concurs with our observations.
Regarding the use of irrigation, Kim et al. [1] reported a higher recurrence rate in a 114-case saline irrigation group with closed drainage than in a 38-case non-irrigation group with closed drainage. Conversely, Ishibashi et al. [14], Jang et al. [8], and Lee et al. [5] reported better prognoses after irrigation. The present study also showed that the recurrence rate was significantly lower after intraoperative irrigation.
Based on our observation that intraoperative irrigation reduced CSDH recurrence, we suggest that additional research is needed to optimize the irrigation procedure. Shimamura et al. [11] compared the use of thrombin irrigation in 36 patients and saline irrigation in 43 patients and concluded that irrigation with thrombin solution reduced recurrence. In future research, we intend to investigate the effects of the composition and osmolarity of the irrigation solution on CSDH recurrence.
A number of studies have been conducted to identify factors associated with CSDH recurrence, but the present study is the first to compare the effects of the number of burr-holes and irrigation in a single cohort. However, the present study has the obvious limitations of bias and a small sample size, and is inherently limited by its retrospective, single-center design. A prospective, randomized, controlled study is required to resolve the issues arising from discrepancies in results across studies to enable us to meet the challenge posed by the high recurrence rate after burr-hole craniostomy for CSDH.
CONCLUSION
The incidence of CSDH is certain to increase in parallel with population aging, and ongoing research is therefore required to develop better treatments. In the present study, the overall recurrence rate of CSDH after burr-hole drainage surgery was 18.3%. In patients with a history of preoperative antiplatelet medication use, the recurrence rate was particularly high (53.3%), but other medical comorbidities were not found to be related to recurrence. However, the use of intraoperative irrigation was found to reduce the recurrence rate significantly, from 25.5% to 8.6%, whereas the number of burr-holes did not have any significant effect. Accordingly, we recommend active irrigation during burr-hole craniostomy in patients with CSDH.