Articles
- Page Path
- HOME > J Trauma Inj > Volume 33(3); 2020 > Article
-
Original Article
An Early Experience of Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) in the Republic of Korea: A Retrospective Multicenter Study - Joonhyeon Park, M.D.1, Sung Woo Jang, M.D.1, Byungchul Yu, M.D.2, Gil Jae Lee, M.D., Ph.D.2, Sung Wook Chang, M.D.3, Dong Hun Kim, M.D.4, Ye Rim Chang, M.D., Ph.D.4, Pil Young Jung, M.D., Ph.D.1
-
Journal of Trauma and Injury 2020;33(3):144-152.
DOI: https://doi.org/10.20408/jti.2020.0051
Published online: September 30, 2020
- 4,354 Views
- 108 Download
- 5 Crossref
1Department of Surgery, Trauma Center, Yonsei University Wonju Severance Christian Hospital, Wonju, Korea
2Department of Surgery, Trauma Center, Gachon University Gil Medical Center, Incheon, Korea
3Department of Thoracic and Cardiovascular Surgery, Trauma Center, Dank University Hospital, Cheonan, Korea
4Department of Surgery, Trauma Center, Dankook University Hospital, Cheonan, Korea
- Correspondence to Pil Young Jung, M.D., Ph.D. Regional Trauma Center, Wonju Severance Christian Hospital, Department of Surgery, Yonsei University Wonju College of Medicine, 20 Ilsan-ro, Wonju 26426, Korea Tel: +82-33-741-0573 Fax: +82-33-741-0574 E-mail: surgery4trauma@yonsei.ac.kr
Copyright © 2020 The Korean Society of Trauma
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Purpose
- This retrospective multicenter study analyzed trauma patients who underwent resuscitative endovascular balloon occlusion of the aorta (REBOA) in the Republic of Korea.
-
Methods
- This study was conducted from February 2017 to May 2018 at three regional trauma centers in the Republic of Korea. The patients were divided into two groups (cardiopulmonary resuscitation [CPR] and No-CPR) for comparative analysis based on two criteria (complication and mortality) for logistic regression analysis (LRA).
-
Results
- There were significant differences between the CPR and No-CPR groups in mortality (p=0.003) and treatment administered (p=0.016). By LRA for complications, total occlusion has significantly lesser risk than intermittent or partial occlusion in both univariate (odds ratio [OR] 0.06, 95% confidence interval [CI] 0.00-0.36, p=0.01) and multivariate (OR 0.05, 95% CI 0.00-0.38, p=0.01) analyses. The Rescue had a higher risk than the Coda or Reliant in univariate analysis (OR 4.91, 95% CI 1.14-34.25, p=0.05); however, it was not statistically significant in multivariate analysis (OR 6.98, 95% CI 1.03-74.52, p=0.07). By LRA for mortality, the CPR group was the only variable that had a significantly higher risk of mortality than the No-CPR group in both univariate (OR 17.59, 95% CI 3.05-335.25, p=0.01), and multivariate (OR 24.92, 95% CI 3.77-520.51, p=0.01) analyses.
-
Conclusions
- This study was conducted in the early stages of REBOA implementation in the Republic of Korea and showed conflicting results from studies conducted by multiple institutions. Therefore, additional research with more accumulated data is needed.
- In trauma patients, hemorrhage is one of the most fatal conditions, and it is the second leading cause of traumatic mortality [1]. A total of 30-40% of traumatic patients have died from hemorrhage [2]. Worldwide, 1,481,700 people die from traumatic hemorrhage yearly, and the years of life lost from traumatic hemorrhage are 74,568,000 years [3].
- Resuscitative endovascular balloon occlusion of the aorta (REBOA) has been developed to control hemodynamically unstable hemorrhagic shock patients and to maintain brain and coronary perfusion [4,5]. Emergency resuscitative thoracotomy (ERT), which was previously performed, can be indicated for a single penetrating injury; however, for blunt injuries, there are many debates on performing ERT [6]. Some authors argue that REBOA can replace ERT in select cases [4,7]. In places, such as the Republic of Korea, where most traumatic patients experience blunt traumas (90.8%), REBOA is becoming important for hemorrhagic shock patients [8]. However, REBOA has several disadvantages [9]: 1) It is extremely time-dependent. 2) It has limited indications in patients with abdominal or pelvic hemorrhage who have a detectable pulse but whose systolic blood pressure remains 80 mmHg or less despite resuscitative efforts [10]. 3) It has many complications, such as distal ischemia and mortality. Nevertheless, because REBOA can play an important role in saving the time required to proceed to the next stage of treatment in blunt trauma patients, discussions to find an appropriate indication for REBOA and reduce its complications are under way.
- As a result, in this multicenter retrospective study, we analyzed trauma patients who underwent REBOA according to their mortality, development of complications, and cardiopulmonary resuscitation (CPR). Furthermore, we tried to identify other variables that can affect the risk of complications and mortality. We hypothesized that the type of REBOA and type of catheter used may affect the risk for complications and mortality.
- Group for Resuscitative Endovascular and Advanced treatment on Trauma (GREAT)
- GREAT is an academic society in the Republic of Korea that studies endovascular treatment of trauma, including REBOA, and conducts research and education. The first meetings began in December 2016, and the data collection for this study was conducted by GREAT. GREAT has developed an education program for REBOA called ET-REBOA. ET-REBOA was first started in May 2018 and is currently being implemented as a Korean Association for Research, Procedures, and Education on Trauma (KARPET) education program (http://karpet.or.kr).
INTRODUCTION
- Population
- This was a retrospective multicenter study conducted from February 2017 to May 2018 at three regional trauma centers belonging to tertiary medical institutions in the Republic of Korea. We collected data of patients who underwent REBOA using the registry of Yonsei University Wonju Severance Christian Hospital, Dankook University Hospital, and Gachon University Gil Medical Center. The patients were divided into two groups (CPR and No-CPR) for comparative analysis and were divided based on two criteria (survival and mortality, occurrence and nonoccurrence of complication) for logistic regression analysis (LRA). The CPR group comprised patients who received CPR, while the No-CPR group included those who did not receive CPR. The demographic data, injury severity score (ISS), injury type, reason for REBOA, access method (cut down, palpitation, ultrasonography), access site, confirmation of the balloon position, type of catheter, type of REBOA, zone of REBOA, time of occlusion, treatment after REBOA, name of the provider, and information on development of complications and mortality was obtained from the electronic medical records of the study patients. The mechanisms of injury were classified as blunt or penetrating. The reasons for REBOA were classified as low extremity or pelvis injury, abdomen or chest injury, and multiple injuries. The treatment after REBOA was classified as surgery, angioembolization, both surgery and angioembolization, and no treatment.
- REBOA
- All patients received REBOA in the hospital. In most cases, REBOA was performed based on the judgment of the trauma surgeon on duty, but in two cases, it was performed by an emergency physician or vascular surgeon. We used a Coda® balloon 14 Fr catheter (Cook Medical, Bloomington, USA), Reliant® balloon 12 Fr catheter (Medtronic, Minneapolis, USA), and Rescue balloon® 7 Fr catheter (Tokai Medical Products, Aichi, Japan). In all cases, the access site was the femoral artery, and we used both the left and right femoral arteries. The REBOA zone was confirmed via radiography, C-arm, and ultrasonography, but two cases were not confirmed (blind). Total and partial or intermittent occlusion was performed depending on the patient’s condition. The duration of REBOA was measured from the first balloon inflation to the final deflation.
- Statistical analysis
- All statistical analyses were performed using R Statistical Software (version 3.6.3; R Foundation for Statistical Computing, Vienna, Austria). For the comparison of trauma patients who underwent REBOA with or without CPR, the Student’s t-test was used for continuous variables, based on the normal distribution, which was confirmed using the Shapiro-Wilk test, and the Fisher exact test was used to compare categorical variables. Two LRA models were created with mortality and complications as dependent variables. All LRA were performed as univariate and multivariate analyses. The independent variables of these models were age, sex, ISS, type of REBOA, type of catheter, and CPR. All results of LRA were expressed as odds ratios (ORs) and 95% confidence intervals (CIs). For all statistical analyses, p<0.05 was considered statistically significant.
METHODS
- Patient selection and characteristics
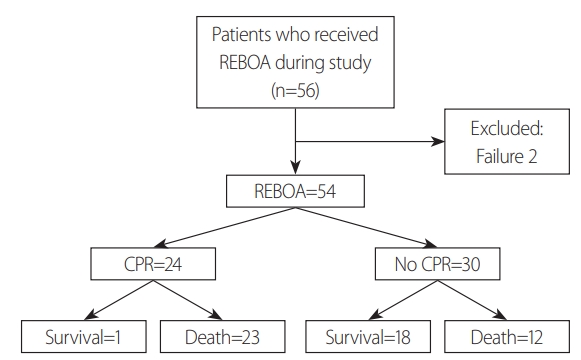
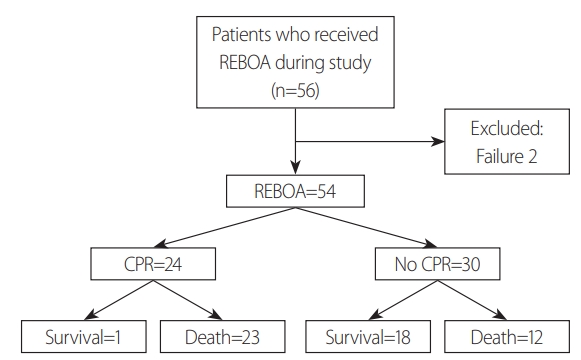
- The flowchart of this study is summarized in Fig 1. During the study period, 56 patients received REBOA. Two patients were excluded due to failure; consequently, 54 patients were eligible for this study. Twenty-four patients received CPR. Among them, only one patient survived (4.2%). In the No-CPR group, 18 patients survived (60.0%). A total of 19 patients survived (35.2%), and 35 patients died (64.8%). Mortality was significantly higher in the CPR group (p=0.003).
- Other characteristics of patients according to the CPR status are summarized in Table 1. There were no significant differences in sex (p=0.729), age (p=0.299), ISS (p=0.755), injury type (p=1.000), multiple injury (p=1.000), low extremity injury (p=0.842), pelvic bone fracture (p=0.520), intra-abdominal injury (p=1.000), intra-chest injury (p=0.842), access method (p=0.652), access site (p=0.927), confirmation of balloon position (p=0.337), type of catheter (p=0.740), type of REBOA (p=0.207), zone (p=0.877), time of occlusion (p=0.494), provider (p=0.359), and occurrence of complications (p=0.282) between the CPR and No-CPR groups. Only one patient received REBOA due to penetrating injury. REBOA balloons were confirmed by radiography in most cases (90.7%), and there were two cases in which REBOA balloons were placed in Zone 2. On the other hand, there were significant differences in mortality (p=0.003) and following treatment (p=0.016) between the CPR group and the No-CPR group.
- Logistic regression analysis for complications
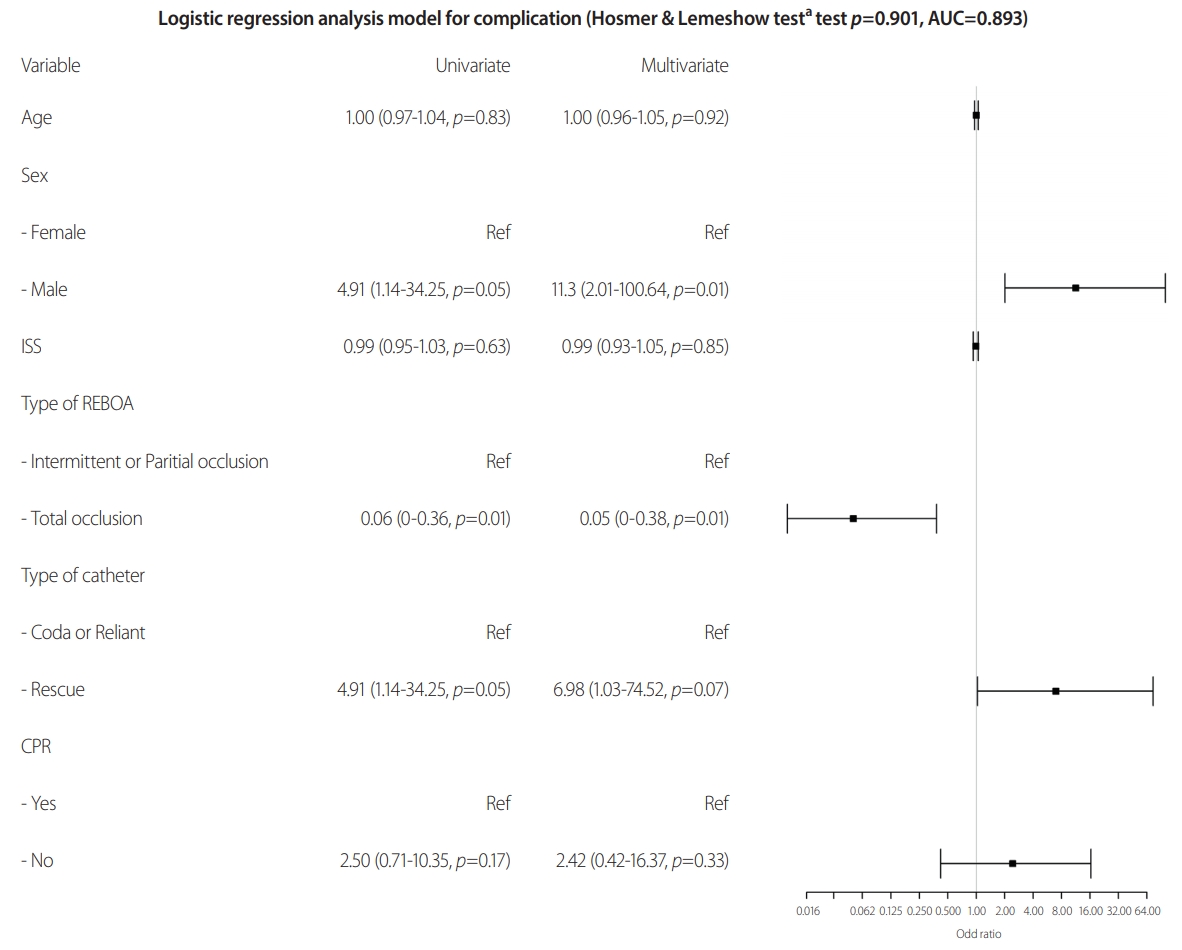
- Univariate and multivariate LRA for the occurrence of complications were performed. Age was not statistically significant in both univariate (OR 1.00, 95% CI 0.97-1.04, p=0.83) and multivariate (OR 1.00, 95% CI 0.96-1.05, p=0.92) analyses. Males had a significantly higher risk of complications than females in both univariate (OR 4.91, 95% CI 1.14-34.25, p=0.05) and multivariate (OR 11.3, 95% CI 2.01-100.64, p=0.01) analyses, and the effect was reinforced in multivariate analysis. ISS was not statistically significant in both univariate (OR 0.99, 95% CI 0.95-1.03, p=0.63) and multivariate (OR 0.99, 95% CI 0.93-1.05, p=0.85) analyses. Total occlusion had a significantly lesser risk than intermittent or partial occlusion in both univariate (OR 0.06, 95% CI 0.00-0.36, p=0.01) and multivariate (OR 0.05, 95% CI 0.00-0.38, p=0.01) analyses, and the effects were similar between univariate and multivariate analyses. The Rescue had a higher risk than Coda or Reliant in univariate analysis (OR 4.91, 95% CI 1.14-34.25, p=0.05), but it was not statistically significant in multivariate analysis (OR 6.98, 95% CI 1.03-74.52, p=0.07). However, it cannot be easily ignored because 95% CI of multivariate analysis does not include 1. Finally, the No-CPR group was not statistically significant compared to the CPR group in both univariate (OR 2.50, 95% CI 0.71-10.35, p=0.17), and multivariate (OR 2.43, 95% CI 0.42-16.37, p=0.33) analyses. The p-value of Hosmer and Lemeshow goodness of fit test for this model was 0.901, and the area under the receiver operating characteristic curve (AUC) was 0.893, which means that this LRA model explains the data of this study well.
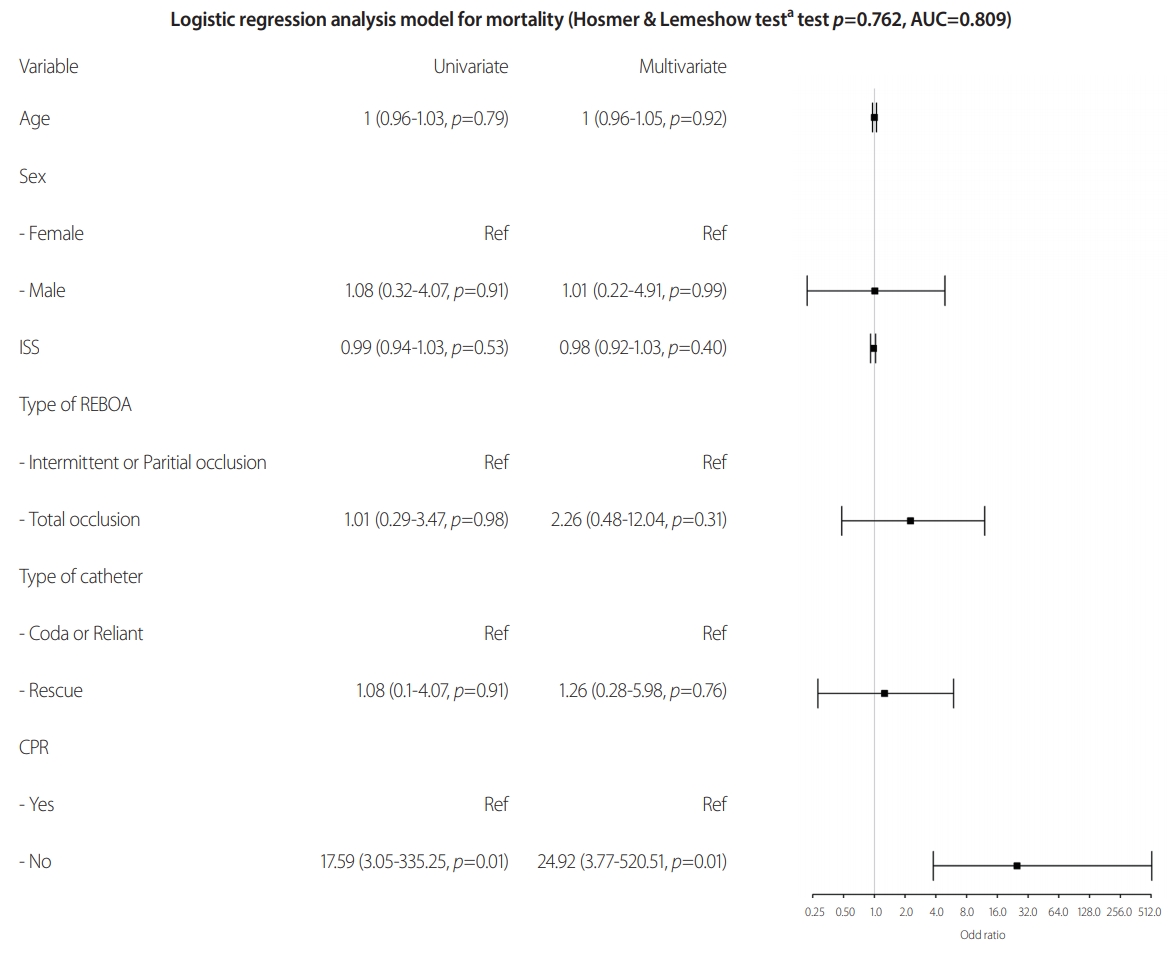
- Logistic regression analysis for mortality
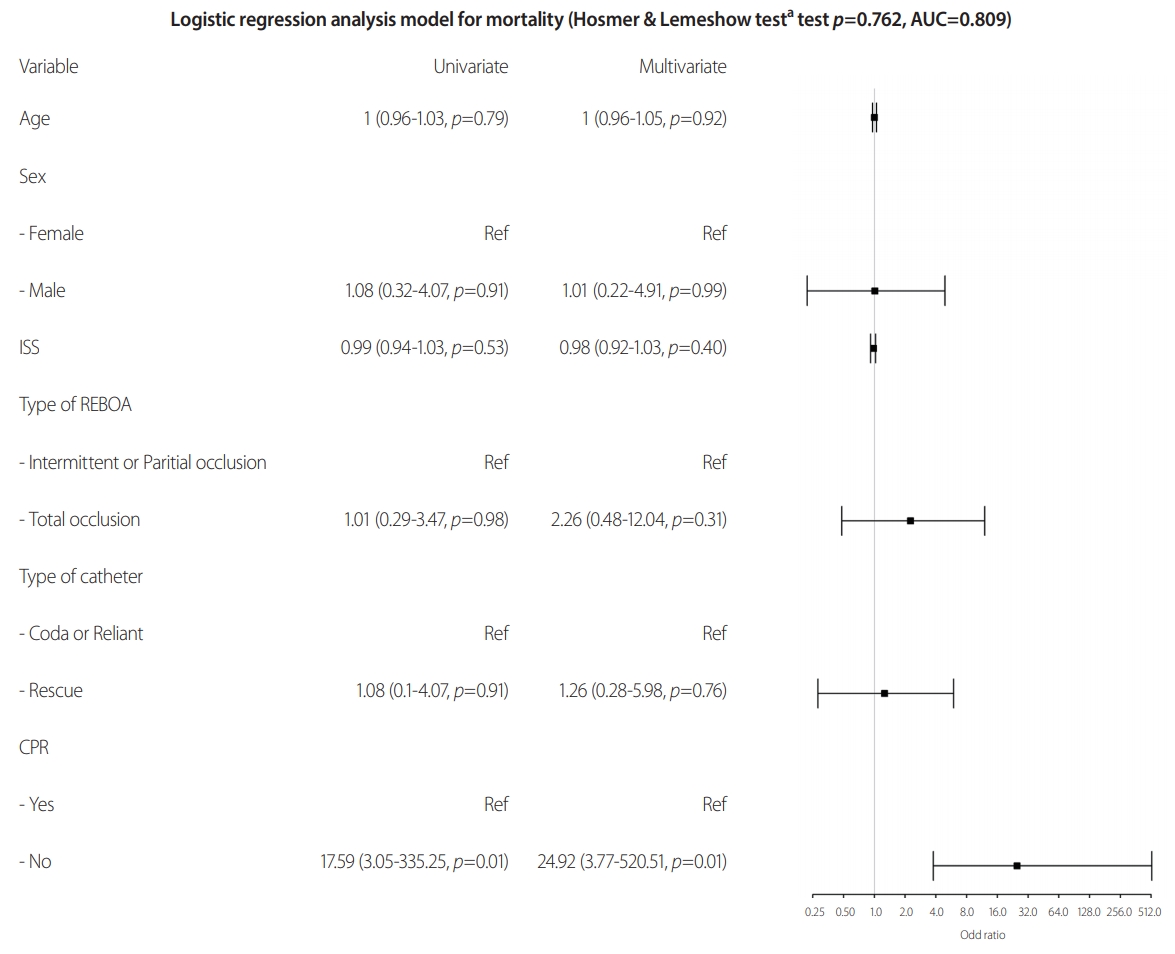
- Univariate and multivariate LRA for mortality were also performed. Age was not statistically significant in both univariate (OR 1.00, 95% CI 0.96-1.03, p=0.79) and multivariate (OR 1.00, 95% CI 0.96-1.05, p=0.92) analyses. Male sex was not statistically significant compared to female sex in both univariate (OR 1.08, 95% CI 0.31-4.07, p=0.91) and multivariate (OR 1.01, 95% CI 0.22-4.91, p=0.99) analyses. ISS was not statistically significant in both univariate (OR 0.99, 95% CI 0.94-1.03, p=0.53) and multivariate (OR 0.98, 95% CI 0.92-1.03, p=0.40) analyses. Total occlusion was not statistically significant compared to intermittent or partial occlusion in both univariate (OR 1.01, 95% CI 0.29-3.47, p=0.98) and multivariate (OR 2.26, 95% CI 0.48-12.04, p=0.31) analyses. Rescue was not statistically significant compared to Coda or Reliant in both univariate (OR 1.08, 95% CI 0.31-4.07, p=0.91) and multivariate (OR 1.26, 95% CI 0.28-5.98, p=0.76) analyses. The CPR group was the only variable that had a significantly higher risk for mortality than the No-CPR group in both univariate (OR 17.59, 95% CI 3.05-335.25, p=0.01) and multivariate (OR 24.92, 95% CI 3.77-520.51, p=0.01) analyses. The p-value of Hosmer and Lemeshow goodness of fit test for this model was 0.762, and AUC was 0.809. Therefore, the LRA model for mortality fits the data of this study.
RESULTS
- When we compared the CPR and No-CPR groups in trauma patients who underwent REBOA within our study, no variables, except mortality and following treatment, showed significant differences between the two groups. Chen et al. [11] reported that only 2.2% of traumatic cardiac arrest patients survived for at least 30 days, and ISS above 16 and total resuscitation length above 20 minutes were unfavorable factors for mortality. In our study, the mean ISS was 34.9±15.0. Consequently, CPR is an independent factor influencing mortality. In the CPR group, six patients could not receive the following treatment because the patients had expired. More patients in the No-CPR group received other treatments, such as surgery, angiographic embolization, or both than those in the CPR group.
- The main reason for REBOA is intra-abdominal injury (57.4%). However, if we check each injury type, pelvic bone fracture (44.4%) was the most common reason for REBOA, and liver injury was the second most common reason. The injury type distribution by the detailed organ is described in Table 2. Fourteen patients (25.9%) had multiple organ injuries, and there was no significant difference between the CPR and the No-CPR groups (p=1.000). The majority of our cases showed intra-abdominal organ injury or pelvic bone fracture. In 3 cases we performed REBOA on patients with lung injury. Two of them had multiple organ (spleen, liver, and lung) injuries, and the other had solitary lung injury. REBOA is indicated mostly in patients with life-threatening hemorrhagic injuries below the diaphragm [12], and the performance of REBOA in thoracic trauma patients with or without other torso injuries has been debated [13]. Ordoñez et al. [14] suggested that the combination of REBOA and ERT could be useful in patients with non-compressible torso hemorrhage secondary to penetrating chest trauma in their 7-case series report. However, in our study, all patients with lung injury were injured from blunt trauma; therefore, it is better to be careful about implementation of REBOA in patients with thoracic injuries.
- Fourteen patients developed complications, as described in Table 3. Postoperative bleeding was the highest in four cases, followed by lower limb ischemia in two cases. There was one case each for bowel ischemia, sigmoid colon perforation, acute respiratory distress syndrome, lung atelectasis, pleural effusion, pulmonary thromboembolism, stress-induced cardiomyopathy, and pseudoaneurysm. There are many complications associated with REBOA. The reported complications of REBOA included femoral arterial complications (disruption, dissection, pseudoaneurysm, hematoma, thromboembolism), extremity ischemia, aortoiliac complication (intimal tear, dissection, rupture), and bowel ischemia [12,15]. The conditions in which complications occur during REBOA implementation are: 1) the physical damage inflicted on the accessing vessel (femoral artery or iliac vessels); and 2) ischemia and inflammation caused by blockage of downstream blood flow [15,16]. Vessels can be injured by the catheter itself or by overinflation of the REBOA balloon. Sadeghi et al. [16] reported that REBOA could cause severe systemic and intra-abdominal metabolic disturbances, organ damage, and inflammatory activation at 30 minutes of occlusion in a non-hemorrhagic porcine model.
- In this study, we attempted to identify the variables that affect the occurrence of complications (Fig. 2). In the LRA model, the occurrence of the complication is the dependent variable, and male sex and total occlusion have a statistically significant effect. However, this result is different from what we hypothesized. Males tend to have a higher risk of complications than females. This may have resulted from a bias that may have occurred during collection of data or due to the small amount of data (total number of patients was 54). In other studies, there is no evidence that males have a higher risk of occurrence of complications [13,15,17]. The judgment of this phenomenon should be withheld until more data is accumulated. The total occlusion of the REBOA balloon has a protective effect on complications than intermittent or partial occlusion. Usually, total occlusion is known to have a higher ischemic burden than partial occlusion [18]. The current guideline for REBOA recommends that total occlusion time in Zone 1 does not exceed 30-45 minutes [19]. However, there were three patients with ischemic complications in this study who received partial or intermittent occlusive REBOA, two of which were in Zone 3 and the other was in Zone 1. These ischemic complications occurred in a relatively early period of this study. It seems to be the complication caused by the patient’s condition or procedural immaturity, rather than problems associated with the type of REBOA. There was only one case in which the complication occurred in total occlusion. This result needs to be analyzed by considering the time that has been occluded rather than the REBOA type, and follow-up studies with data on the proficiency of REBOA and how to implement REBOA is also needed.
- The type of REBOA catheter is not statistically significant for the LRA model for complications. However, considering the 95% CI of this variable, Rescue catheters may have a dangerous effect on the occurrence of complications. The Rescue catheter is a 7 Fr catheter that reduces access-related complications and is safer than the previously used thick catheter [9,20,21]. Therefore, it cannot be concluded that the Rescue catheter has a dangerous effect on the occurrence of complications. During the study period, the Rescue catheter was used relatively later and had the largest number. Therefore, this result should be analyzed considering the time and frequency of use. Accordingly, it seems that this phenomenon is the result of insufficient proficiency in the overall REBOA procedure.
- In the LRA model for death, we could not find any statistically significant variables except whether CPR was performed (Fig. 3). It should be considered that CPR itself is a powerful predictor of death, and REBOA is being implemented to buy time for the next treatment in patients with a high risk of death [9,22,23]. Therefore, further research with more accumulated data is necessary.
DISCUSSION
- REBOA is a technique that can improve hemodynamic stability in patients with life-threatening hemorrhagic shock. It seems that it can replace ERT in selective cases, but exact indications and protocols for REBOA have not been established. This study was conducted in the early stages of REBOA implementation in the Republic of Korea and showed conflicting results from studies conducted by multiple institutions. Therefore, additional research with more accumulated data is needed. Establishing appropriate protocols for REBOA and training for physicians is necessary.
CONCLUSION
| Total (n=54) | CPR (n=24) | No-CPR (n=30) | p-value | |
|---|---|---|---|---|
| Sex | 0.729 | |||
| Male | 34 (63.0) | 14 (58.3) | 20 (66.7) | |
| Female | 20 (37.0) | 10 (41.7) | 10 (33.3) | |
| Age | 50.1±18.7 | 53.1±18.0 | 47.8±19.2 | 0.299 |
| ISS | 34.9±15.0 | 34.2±15.6 | 35.5±14.7 | 0.755 |
| Injury type | 1.000 | |||
| Blunt | 53 (98.1) | 24 (100.0) | 29 (96.7) | |
| Penetrating | 1 (1.9) | 0 (0.0) | 1 (3.3) | |
| Reason of REBOAa | ||||
| Multiple injury | 14 (25.9) | 7 (29.2) | 7 (23.3) | 1.000 |
| Low extremity | 3 (5.6) | 2 (8.3) | 1 (3.3) | 0.842 |
| Pelvic bone fracture | 24 (44.4) | 9 (37.5) | 15 (50.0) | 0.520 |
| Intra-abdominal injury | 31 (57.4) | 14 (58.3) | 17 (56.7) | 1.000 |
| Intra-chest injury | 3 (5.6) | 2 (8.3) | 1 (3.3) | 0.842 |
| Access method | 0.652 | |||
| Cut down | 1 (1.9) | 0 (0.0) | 1 (3.3) | |
| Palpitation | 49 (90.7) | 22 (91.7) | 27 (90.0) | |
| Ultrasonography | 4 (7.4) | 2 (8.3) | 2 (6.7) | |
| Access site | 0.927 | |||
| Right femoral artery | 30 (55.6) | 14 (58.3) | 16 (53.3) | |
| Left femoral artery | 24 (44.4) | 10 (41.7) | 14 (46.7) | |
| Balloon position confirm | 0.337 | |||
| Blind | 2 (3.7) | 2 (8.3) | 0 (0.0) | |
| C-arm | 1 (1.9) | 0 (0.0) | 1 (3.3) | |
| Ultrasonography | 2 (3.7) | 1 (4.2) | 1 (3.3) | |
| X-ray | 49 (90.7) | 21 (87.5) | 28 (93.3) | |
| Type of catheter | 0.740 | |||
| CODAb | 6 (11.1) | 3 (12.5) | 3 (10.0) | |
| RELIANTc | 14 (25.9) | 5 (20.8) | 9 (30.0) | |
| RESCUEd | 34 (63.3) | 16 (66.7) | 18 (60.0) | |
| Type of REBOA | 0.207 | |||
| Partial or Intermittent | 31 (57.4) | 11 (45.8) | 20 (66.7) | |
| Total occlusion | 23 (42.6) | 13 (54.2) | 10 (33.3) | |
| Zone | 0.877 | |||
| 1 | 32 (59.3) | 15 (62.5) | 17 (56.7) | |
| 2 | 2 (3.7) | 1 (4.2) | 1 (3.3) | |
| 3 | 20 (37.0) | 8 (33.3) | 12 (40.0) | |
| Time of occlusion | 151.4±267.0 | 185.1±357.2 | 123.5±163.2 | 0.494 |
| Followed treatment | 0.016 | |||
| No | 6 (11.1) | 6 (25.0) | 0 (0.0) | |
| Angioembolization | 7 (13.0) | 1 (4.2) | 6 (20.0) | |
| Surgery | 38 (70.4) | 16 (66.7) | 22 (73.3) | |
| Angio and surgery | 3 (5.6) | 1 (4.2) | 2 (6.7) | |
| Provider | 0.359 | |||
| Emergency physician | 1 (1.9) | 0 (0.0) | 1 (3.3) | |
| Vascular surgeon | 1 (1.9) | 1 (4.2) | 0 (0.0) | |
| Trauma surgeon | 52 (96.3) | 23 (95.8) | 29 (96.7) | |
| Complication | 14 (25.9) | 4 (16.7) | 10 (33.3) | 0.282 |
| Mortality | 35 (64.8) | 23 (95.8) | 12 (40.0) | 0.003 |
Values are presented as mean±standard deviation or number (%).
CPR: cardiopulmonary resuscitation, ISS: injury severity score, REBOA: resuscitative endovascular balloon occlusion of the aorta.
a Duplicated.
b Coda® balloon 14 Fr catheter (Cook Medical, Bloomington, USA).
c Reliant® balloon 12 Fr catheter (Medtronic, Minneapolis, USA).
d Rescue balloon® 7 Fr catheter (Tokai Medical Products, Aichi, Japan).
| Injured organ (duplicated) | Number |
|---|---|
| Intra-abdominal organ | |
| Liver | 15 |
| Mesentery | 11 |
| Kidney | 5 |
| Spleen | 5 |
| Inferior vena cava | 2 |
| Lung | 3 |
| Pelvic bone fracture | 24 |
| Lower extremity | 3 |
| Multiple organ injury | 14 |
- 1. Tien HC, Spencer F, Tremblay LN, Rizoli SB, Brenneman FD. Preventable deaths from hemorrhage at a level I Canadian trauma center. J Trauma 2007;62:142–6. ArticlePubMed
- 2. Kauvar DS, Lefering R, Wade CE. Impact of hemorrhage on trauma outcome: an overview of epidemiology, clinical presentations, and therapeutic considerations. J Trauma 2006;60(Suppl 6):S3–11. ArticlePubMed
- 3. Cannon JW. Hemorrhagic shock. N Engl J Med 2018;378:370–9. ArticlePubMed
- 4. Brenner M, Inaba K, Aiolfi A, DuBose J, Fabian T, Bee T, et al. Resuscitative endovascular balloon occlusion of the aorta and resuscitative thoracotomy in select patients with hemorrhagic shock: early results from the american association for the surgery of trauma’s aortic occlusion in resuscitation for trauma and acute care surgery registry. J Am Coll Surg 2018;226:730–40. ArticlePubMed
- 5. Darrabie MD, Croft CA, Brakenridge SC, Mohr AM, Rosenthal MA, Mercier NR, et al. Resuscitative endovascular balloon occlusion of the aorta: implementation and preliminary results at an academic level I trauma center. J Am Coll Surg 2018;227:127–33. ArticlePubMed
- 6. Segalini E, Di Donato L, Birindelli A, Piccinini A, Casati A, Coniglio C, et al. Outcomes and indications for emergency thoracotomy after adoption of a more liberal policy in a western European level 1 trauma centre: 8-year experience. Updates Surg 2019;71:121–7. ArticlePubMedPDF
- 7. Moore LJ, Brenner M, Kozar RA, Pasley J, Wade CE, Baraniuk MS, et al. Implementation of resuscitative endovascular balloon occlusion of the aorta as an alternative to resuscitative thoracotomy for noncompressible truncal hemorrhage. J Trauma Acute Care Surg 2015;79:523–30; discussion 530. ArticlePubMed
- 8. Byun CS, Park IH, Oh JH, Bae KS, Lee KH, Lee E. Epidemiology of trauma patients and analysis of 268 mortality cases: trends of a single center in Korea. Yonsei Med J 2015;56:220–6. ArticlePubMed
- 9. Chung JS, Kim OH, Kim S, Jang JY, An GJ, Jung PY. Resuscitative endovascular balloon occlusion of the aorta in impending traumatic arrest: is it effective. J Trauma Inj 2020;33:23–30. ArticlePDF
- 10. Biffl WL, Fox CJ, Moore EE. The role of REBOA in the control of exsanguinating torso hemorrhage. J Trauma Acute Care Surg 2015;78:1054–8. ArticlePubMed
- 11. Chen YC, Wu KH, Hsiao KY, Hung MS, Lai YC, Chen YS, et al. Factors associated with outcomes in traumatic cardiac arrest patients without prehospital return of spontaneous circulation. Injury 2019;50:4–9. Article
- 12. Brenner M, Bulger EM, Perina DG, Henry S, Kang CS, Rotondo MF, et al. Joint statement from the American College of Surgeons Committee on Trauma (ACS COT) and the American College of Emergency Physicians (ACEP) regarding the clinical use of resuscitative endovascular balloon occlusion of the aorta (REBOA). Trauma Surg Acute Care Open 2018;3:e000154. ArticlePubMedPMC
- 13. Bekdache O, Paradis T, Shen YBH, Elbahrawy A, Grushka J, Deckelbaum D, et al. Resuscitative endovascular balloon occlusion of the aorta (REBOA): indications: advantages and challenges of implementation in traumatic non-compressible torso hemorrhage. Trauma Surg Acute Care Open 2019;4:e000262. ArticlePubMedPMC
- 14. Ordoñez CA, Parra MW, Manzano-Nunez R, Herrera-Escobar JP, Serna JJ, Rodriguez Ossa P, et al. Intraoperative combination of resuscitative endovascular balloon occlusion of the aorta and a median sternotomy in hemodynamically unstable patients with penetrating chest trauma: is this feasible. J Trauma Acute Care Surg 2018;84:752–7. ArticlePubMed
- 15. Ribeiro Junior MAF, Feng CYD, Nguyen ATM, Rodrigues VC, Bechara GEK, de-Moura RR, et al. The complications associated with resuscitative endovascular balloon occlusion of the aorta (REBOA). World J Emerg Surg 2018;13:20. ArticlePubMedPMCPDF
- 16. Sadeghi M, Dogan EM, Karlsson C, Jansson K, Seilitz J, Skoog P, et al. Total resuscitative endovascular balloon occlusion of the aorta causes inflammatory activation and organ damage within 30 minutes of occlusion in normovolemic pigs. BMC Surg 2020;20:43. ArticlePubMedPMCPDF
- 17. Osborn LA, Brenner ML, Prater SJ, Moore LJ. Resuscitative endovascular balloon occlusion of the aorta: current evidence. Open Access Emerg Med 2019;11:29–38. ArticlePubMedPMC
- 18. Hoareau GL, Tibbits EM, Beyer CA, Simon MA, DeSoucy ES, Faulconer ER, et al. Resuscitative endovascular balloon occlusion of the aorta: review of the literature and applications to veterinary emergency and critical care. Front Vet Sci 2019;6:197. ArticlePubMedPMC
- 19. Otsuka H, Sato T, Sakurai K, Aoki H, Yamagiwa T, Iizuka S, et al. Effect of resuscitative endovascular balloon occlusion of the aorta in hemodynamically unstable patients with multiple severe torso trauma: a retrospective study. World J Emerg Surg 2018;13:49. ArticlePubMedPMCPDF
- 20. Matsumura Y, Matsumoto J, Kondo H, Idoguchi K, Ishida T, Kon Y, et al. Fewer REBOA complications with smaller devices and partial occlusion: evidence from a multicentre registry in Japan. Emerg Med J 2017;34:793–9. ArticlePubMed
- 21. Teeter WA, Matsumoto J, Idoguchi K, Kon Y, Orita T, Funabiki T, et al. Smaller introducer sheaths for REBOA may be associated with fewer complications. J Trauma Acute Care Surg 2016;81:1039–45. ArticlePubMed
- 22. Özkurtul O, Staab H, Osterhoff G, Ondruschka B, Höch A, Josten C, et al. Technical limitations of REBOA in a patient with exsanguinating pelvic crush trauma: a case report. Patient Saf Surg 2019;13:25. ArticlePubMedPMCPDF
- 23. Tiba MH, McCracken BM, Cummings BC, Colmenero CI, Rygalski CJ, Hsu CH, et al. Use of resuscitative balloon occlusion of the aorta in a swine model of prolonged cardiac arrest. Resuscitation 2019;140:106–12. ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Complications associated with the use of resuscitative endovascular balloon occlusion of the aorta (REBOA): an updated review
Marcelo Augusto Fontenelle Ribeiro Junior, Salman M Salman, Sally M Al-Qaraghuli, Farah Makki, Riham A Abu Affan, Shahin Reza Mohseni, Megan Brenner
Trauma Surgery & Acute Care Open.2024; 9(1): e001267. CrossRef - Contemporary Utilization and Outcomes of Resuscitative Endovascular Balloon Occlusion of the Aorta for Traumatic Noncompressible Torso Hemorrhage in Korea: A Retrospective Multi-Center Study
Yoonjung Heo, Sung Wook Chang, Byungchul Yu, Byung Hee Kang, Pil Young Jung, Kyounghwan Kim, Dong Hun Kim
Journal of Acute Care Surgery.2024; 14(1): 16. CrossRef - Editor's Choice – Systematic Review and Meta-Analysis of Lower Extremity Vascular Complications after Arterial Access for Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA): An Inevitable Concern?
Megan Power Foley, Stewart R. Walsh, Nathalie Doolan, Paul Vulliamy, Morgan McMonagle, Christopher Aylwin
European Journal of Vascular and Endovascular Surg.2023; 66(1): 103. CrossRef - Early experience with resuscitative endovascular balloon occlusion of the aorta for unstable pelvic fractures in the Republic of Korea: a multi-institutional study
Dong Hun Kim, Jonghwan Moon, Sung Wook Chang, Byung Hee Kang
European Journal of Trauma and Emergency Surgery.2023; 49(6): 2495. CrossRef - Comparison between external fixation and pelvic binder in patients with pelvic fracture and haemodynamic instability who underwent various haemostatic procedures
Ji Young Jang, Keum Soek Bae, Byung Hee Kang, Gil Jae Lee
Scientific Reports.2022;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite