Articles
- Page Path
- HOME > J Trauma Inj > Volume 35(2); 2022 > Article
-
Case Report
Thoracoabdominal injury with evisceration from a chainsaw assault: a case report -
Babatunde Abayomi Salami, FMCS, FWACS
 , Babatunde Adeteru Ayoade, FWACS, FRCS, El-Zaki Abdullahi Shomoye, FMCS, Chigbundu Collins Nwokoro, FWACS
, Babatunde Adeteru Ayoade, FWACS, FRCS, El-Zaki Abdullahi Shomoye, FMCS, Chigbundu Collins Nwokoro, FWACS -
Journal of Trauma and Injury 2022;35(2):118-122.
DOI: https://doi.org/10.20408/jti.2021.0012
Published online: May 11, 2022
- 5,751 Views
- 79 Download
Department of Surgery, Olabisi Onabanjo University Teaching Hospital, Sagamu, Nigeria
- Correspondence to Babatunde Abayomi Salami, FMCS Department of Surgery, Olabisi Onabanjo University Teaching Hospital, P.M.B. 2001, Hospital Road, Sagamu 121102, Nigeria Tel: +234-805-886-2281 E-mail: salami.babatunde@oouagoiwoye.edu.ng
Copyright © 2022 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- The usual cause of penetrating thoracoabdominal injuries with evisceration are stab wounds with knives and other sharp weapons used during fights and conflicts. Evisceration of the abdominal viscera as a result of trauma, with its attendant morbidity and mortality, requires early intervention. Gunshot wounds can also cause penetrating thoracoabdominal injuries. We report the case of a 52-year-old male patient, a worker at a timber-processing factory, who was assaulted with a chainsaw by his colleague following a disagreement. He was seen at the accident and emergency department of Olabisi Onabanjo University Teaching Hospital, Sagamu, Nigeria with a thoracoabdominal injury about 1.5 hours after the attack. He had a left thoracoabdominal laceration with abdominal evisceration and an open left pneumothorax. He was managed operatively, made a full recovery, and was discharged 16 days after admission. He was readmitted 4 months after the initial surgery with acute intestinal obstruction secondary to adhesions. He underwent exploratory laparotomy and adhesiolysis. He made an uneventful recovery and was discharged on the 9th postoperative day for subsequent follow-up.
- Thoracoabdominal injuries may be blunt or penetrating. Penetrating thoracoabdominal injuries (PTAIs) are associated with a high mortality rate (up to 31%) [1]. The concern is that diaphragmatic and pleural breach may lead to contamination, infection, and collection, resulting in morbidity and mortality. PTAIs affect two anatomical cavities, and the difficulty of surgical management may therefore be considerable, depending on the organs injured. Diaphragmatic injuries associated with penetrating PTAIs can cause severe morbidity and mortality if undetected. Laparoscopy is therefore a useful tool for detecting diaphragmatic injuries in penetrating thoracoabdominal stab wounds [2]. Patients with PTAIs have an overall incidence of diaphragmatic injuries of about 42% [3].
- Patients with major thoracic vessel injuries or aortic injuries have a lower chance of survival and often die before arrival at the hospital. The trajectory of the offending weapon or missile determines the organs involved, especially if it traverses the diaphragm. Stab wounds are a common cause of abdominal evisceration [4,5] and the knife is the commonest offending weapon apart from broken bottles and glass [6].
- A chainsaw is a hand-held powered equipment used by loggers in the timber industry for felling trees and cutting timber. It is a commonly used tool that has a risk of causing severe injuries. It cuts with a set of teeth attached to a rotating chain driven along a guide bar. Chainsaws were found to be the cause of about 15.5% of severe injuries in a work-related setting [7]. Injuries from chainsaws are usually accidental. The feet are the most frequently seriously injured part of the body, while the torso, shoulder, and neck are the least injured [8]. A literature search did not reveal any cases of combined thoracoabdominal injuries with evisceration from either accidental chainsaw injuries or chainsaw assault. We therefore report the case of a patient who was assaulted on the torso with a chainsaw at a timber-processing factory, resulting in a thoracoabdominal injury with abdominal evisceration and open pneumothorax.
INTRODUCTION
- The patient was a 52-year-old worker at a timber logging factory who was assaulted by a coworker on the torso with a chainsaw following a conflict. He was seen at the emergency department of Olabisi Onabanjo University Teaching Hospital, Sagamu, Nigeria about 1.5 hours after the injury (Fig. 1). He had lost an estimated 500 mL of blood. His last meal was about 7 hours before the injury. He had no known comorbidities, such as diabetes mellitus or hypertension.
- The patient was found to be a middle-aged man, conscious, and with a pale complexion, with blood-stained clothing wrapped over the chest and over the exposed abdominal viscera (Fig. 1). His hemodynamic status was stable, with a heart rate of 96 beats/min, and blood pressure of 110/70 mmHg. He was tachypneic, with a respiratory rate of 36 breaths/min. The packed cell volume was 33%, serum electrolytes and urea were normal, and one unit of whole blood was cross-matched.
- There was a ragged spiral laceration extending from the lateral aspect of the lower left hemithorax to about 4 cm to the left of the umbilicus. Evisceration of the stomach, small bowel, and transverse colon was observed (Fig. 2). A laceration of the stomach discharged gastric contents, which stained the eviscerated organs. There was no active bleeding except for mild bleeding from the edges of the thoracoabdominal wound, which penetrated the left thoracic cavity. There was tenderness and crepitation over the left lower ribs. Reduced movement of the left hemithorax with respiration was observed, and no air entry was noted in the middle and lower chest zones. There were no other associated external injuries.
- He was commenced on intravenous fluids, nasogastric intubation, and urethral catheterization. The exposed viscera were irrigated with normal saline and packed with gauze. He was commenced on intravenous ceftriaxone 1 g at 12-hour intervals and intravenous metronidazole (500 mg) at 8-hour intervals. His initial oxygen saturation level (SpO2) was 92% and he was commenced on oxygen using a nasal cannula with prongs. He was moved to the operating room for exploration and repair after a thorough assessment.
- Operative findings and treatment
- Exploration was carried out through the penetrating thoracoabdominal laceration caused by the chainsaw. There was no need to extend the thoracoabdominal wound because it was adequate for exploration. The wound measured about 30 cm in length from the lower left chest wall to the left of the midline of about 4 cm from the umbilicus. The eviscerated viscera included the stomach, small bowel, and transverse colon. There was a 4-cm laceration along the greater curvature of the stomach discharging gastric contents. Exploration of the abdomen revealed a small capsular laceration of the spleen on the anterior margin held together by blood clots. There was a laceration of the left hemidiaphragm about 8 cm in length, through which the lower lobe of the lung herniated into the peritoneal cavity. The seventh to 12th ribs were fractured with mild hemothorax.
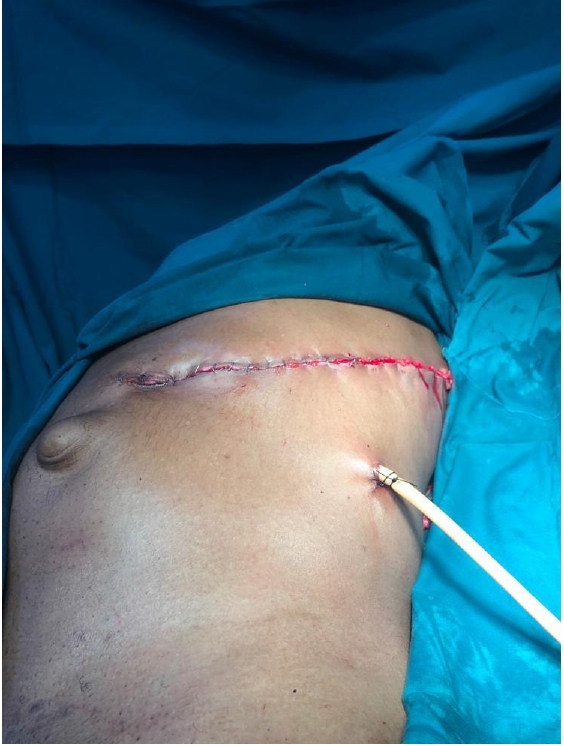
- The eviscerated organs were irrigated copiously with normal saline. The edge of the stomach laceration was freshened before its repair in two layers. The capsular laceration on the spleen was repaired. The left hemothorax was aspirated and the diaphragm repaired. Debridement of the thoracoabdominal wound was carried out before closure in layers, leaving an intraperitoneal drain in situ (Fig. 3). Left closed thoracostomy tube drainage was done and the patient was moved to the intensive care unit for postoperative monitoring after extubation. The estimated blood loss during surgery was about 200 mL and the patient received an intraoperative transfusion with one unit of whole blood. Oxygen supplement was discontinued about 3 hours postoperatively when patient was fully awake and his SpO2 at 4 hours postoperatively was 99% on room air. On postoperative day 2, he was commenced on chest physiotherapy and early mobilization, and his postoperative packed cell volume was 32%. The nasogastric tube was removed on postoperative day 3 when bowel sounds became active, and he was commenced on oral intake. The wound was reviewed on postoperative day 5 (Fig. 4). His chest tube was removed on postoperative day 9 and he was discharged on postoperative day 16 in satisfactory condition.
- The patient presented again 4 months after discharge with features of acute intestinal obstruction. The findings were in keeping with intestinal obstruction secondary to adhesions. He underwent exploratory laparotomy and adhesiolysis and was discharged on postoperative day 9 in satisfactory condition.
CASE REPORT
- This patient was assaulted with a chainsaw, which is not a conventional weapon. Usually, attacks and fights are carried out using knives or broken bottles [6]. A chainsaw is a powered hand-held tool that is capable of accidentally causing severe and devastating traumatic injuries. Severe accidental injuries such as amputations, fractures, and maxillofacial injuries have been reported [9,10]. Deaths from chainsaw accidents have also been reported, although they are rare [11], and suicide using a chainsaw has also been reported [12]. There are published works on accidental chainsaw injuries related to occupational use [7,8,13], but we did not find any previous reports of chainsaw injuries due to assault.
- The risk factors for morbidity and mortality include the length of time between the injury and surgery, and presence of shock at the time of admission [14]. This patient was seen in the accident and emergency department about 1.5 hours after the injury, and underwent surgery about 2 hours later, making the total interval until surgical intervention approximately 3.5 hours. A surgical intervention time of less than 1 hour in patients with abdominal trauma that required surgery was associated with better outcomes [6]. This surgical intervention time of less than 1 hour can be achieved in places where there are efficient helicopter and ambulance services. This patient was hemodynamically stable at the time of admission in the accident and emergency department, and this was because he did not sustain any major vascular injury. This was an important factor that contributed to his recovery. The exposed viscera were covered with gauze soaked in saline to minimize fluid loss and protect the viscera. The successful outcome and recovery of this patient were also due to prompt resuscitation and early operative intervention.
- The extent of the associated chest injury was identified during surgery; the patient underwent diaphragm repair and had left closed thoracostomy tube drainage. The possibility of diaphragmatic injury must always be suspected with PTAIs. This patient received broad-spectrum antibiotics because of the potential contamination of the pleural and peritoneal cavities at the time of injury. The chest tube was left until there was no sign of infection or collection. Intestinal obstruction secondary to adhesions, which occurred 4 months after the initial surgery in this case, is a known complication of exploratory laparotomy [15]. Since a chainsaw can be used as a lethal weapon, workers who use this equipment may require a psychological assessment and background check before employment to prevent this type of incident.
DISCUSSION
-
Ethical statements
This study was approved by the Health Research Ethics Committee of Olabisi Onabanjo University Teaching Hospital (No. OOUTH/HREC/394/2021), in accordance with the principles of the Declaration of Helsinki. Informed consent for publication of the research details and clinical images was obtained from the patient
-
Conflicts of interest
The authors have no conflicts of interest to declare.
-
Funding
None.
-
Author contributions
Conceptualization: BAS; Visualization: BAS, EAS; Writing–original draft: all authors; Writing–review & editing: all authors.
All authors read and approved the final manuscript.
ARTICLE INFORMATION




- 1. Asensio JA, Arroyo H Jr, Veloz W, et al. Penetrating thoracoabdominal injuries: ongoing dilemma-which cavity and when. World J Surg 2002;26:539–43. ArticlePubMed
- 2. Yucel T, Gonullu D, Matur R, et al. Laparoscopic management of left thoracoabdominal stab wounds: a prospective study. Surg Laparosc Endosc Percutan Tech 2010;20:42–5. ArticlePubMed
- 3. Murray JA, Demetriades D, Cornwell EE 3rd, et al. Penetrating left thoracoabdominal trauma: the incidence and clinical presentation of diaphragm injuries. J Trauma 1997;43:624–6. ArticlePubMed
- 4. Shah T. A case report of a paediatric intestinal evisceration by road traffic accident in Nepal. SAJ Case Rep 2017;4:305. Article
- 5. Nagy K, Roberts R, Joseph K, An G, Barrett J. Evisceration after abdominal stab wounds: is laparotomy required? J Trauma 1999;47:622–4. ArticlePubMed
- 6. Osinowo AO, Olusoji OO, Adesanya AA. Abdominal stab wounds in Lagos: a review of fifty cases. Niger Postgrad Med J 2016;23:86–92. ArticlePubMed
- 7. Okokon IB, Asibong UE, Archibong F, Monjok E. Work-related traumatic injury in the paper-producing industry in Nigeria: a case study of the Nigerian newsprint manufacturing company limited, Oku-Iboku, Akwa Ibom State. Fam Med Med Sci Res 2014;3:4. Article
- 8. Parker R, Ashby L. Chainsaw related injuries. COHFE Rep 2005;6:1–4.
- 9. Choi HJ. Case series: successful resuscitation of severe facial injuries caused by a chainsaw. J Trauma Inj 2019;32:168–71. Article
- 10. Cascino F, Pini N, Giovannoni ME, et al. Our experience managing difficult accidental chainsaw trauma. J Craniofac Surg 2019;30:2207–10. ArticlePubMed
- 11. Koehler SA, Luckasevic TM, Rozin L, et al. Death by chainsaw: fatal kickback injuries to the neck. J Forensic Sci 2004;49:345–50. ArticlePubMed
- 12. Tournel G, Dedouit F, Balgairies A, et al. Unusual suicide with a chainsaw. J Forensic Sci 2008;53:1174–7. ArticlePubMed
- 13. Hamming B, Jones C. Epidemiology of chain saw related injuries, United States: 2009 through 2013. Adv Emer Med 2015;2015:1–4. Article
- 14. Gad MA, Saber A, Farrag S, Shams ME, Ellabban GM. Incidence, patterns, and factors predicting mortality of abdominal injuries in trauma patients. N Am J Med Sci 2012;4:129–34. ArticlePubMedPMC
- 15. Barmparas G, Branco BC, Schnuriger B, Lam L, Inaba K, Demetriades D. The incidence and risk factors of post-laparotomy adhesive small bowel obstruction. J Gastrointest Surg 2010;14:1619–28. ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite