
Articles
- Page Path
- HOME > J Trauma Inj > Volume 35(2); 2022 > Article
-
Case Report
Penetrating sacral injury with a metallic pipe: a case report and literature review -
Mahnjeong Ha, MD1
 , Kyoung Hyup Nam, MD1, Jae Hun Kim, PhD2, In Ho Han, PhD1
, Kyoung Hyup Nam, MD1, Jae Hun Kim, PhD2, In Ho Han, PhD1 -
Journal of Trauma and Injury 2022;35(2):131-138.
DOI: https://doi.org/10.20408/jti.2021.0063
Published online: May 11, 2022
- 2,936 Views
- 65 Download
1Department of Neurosurgery and Medical Research Institute, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea
2Department of Trauma and Surgical Critical Care, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea
- Correspondence to In Ho Han, PhD Department of Neurosurgery and Medical Research Institute, Pusan National University Hospital, Pusan National University School of Medicine, 179 Gudeok-ro, Seo-gu, Busan 49241, Korea Tel: +82-51-240-7257 E-mail: farlateral@pusan.ac.kr
Copyright © 2022 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- Other than gunshot injuries, sacral penetrating injuries with a foreign body exiting to the other side are extremely rare. We encountered a case of sacral injury in which a long metallic pipe penetrated from the anus into the lower back of a patient. Since the pelvis contains various organs, management of a penetrating injury requires multidisciplinary treatment involving several medical specialties. Due to the infrequency of this type of injury, there are no definitive guidelines for effective management. We described our experience surgically treating a sacral penetrating injury and conducted a literature review. On this basis, we suggest a surgical strategy for treating this type of injury.
- Penetrating injuries such as stabbing and impalement constitute approximately 0.3% of all spinal cord injuries according to the National Spinal Cord Injury Database, and impalement with a metallic foreign body accounts for only a small proportion of such injuries [1,2]. Penetrating injuries through the torso vary widely depending on the strength of the material. In particular, penetration by a metallic material can strongly impact the bony structure and cause fractures. Surgical treatment for a sacral penetrating injury is difficult due to the anatomical complexity the region and possible combinations of injuries depending on factors such as the foreign object’s material, the trajectory of the foreign object, damage to internal organs and blood vessels, infection, cerebrospinal fluid leakage, and neurological problems.
- We encountered a case involving a sacral penetrating injury through the anus into the lower back, which was treated successfully. Here, we describe our surgical experience, present a literature review, and suggest strategies for managing sacral penetrating injuries.
INTRODUCTION
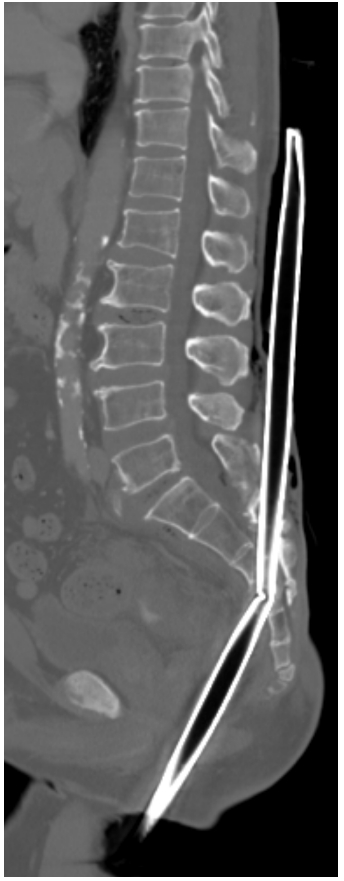
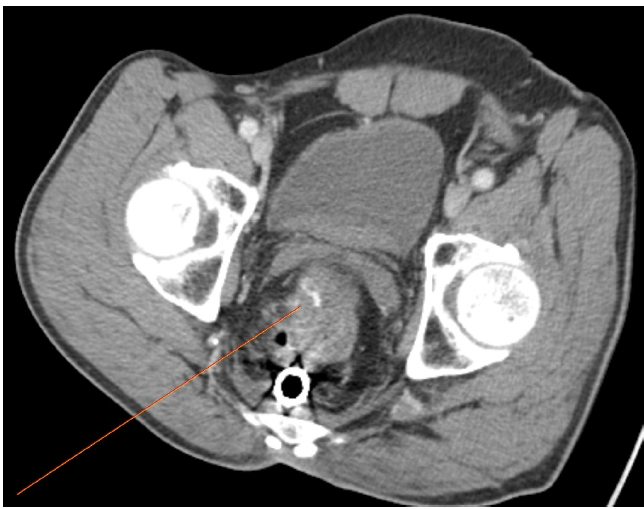
- An 81-year-old male patient who was hospitalized in a nursing hospital was transferred to Pusan National University Hospital. The patient presented with a metallic pipe that pierced through his anus into the lower back of the iliac crest level about 1 hour before admission (Fig. 1). There were no other witnesses of the accident, and the patient stated that he fell in an attempted suicide and was accidentally impaled with an iron pipe. However, the patient could not describe the accident precisely. He patient had been undergoing treatment for depression and had mild cognitive impairment. During the initial physical examination, the patient’s vital signs were stable and laboratory findings were within the normal range, including the hemoglobin level, platelet count, prothrombin time, and activated partial thromboplastin time. Anal tone and reflex could not be determined because of the foreign body, but no other neurologic deficits were identified. A contrast-enhanced computed tomography (CT) scan was performed to accurately examine the internal damage. The CT scan showed that the foreign body entered the anus, perforated the rectum, and entered the body of the fourth right sacral vertebra. The metallic pipe was bent upward inside the sacrum, penetrated the lamina of the second sacrum, and exited through the skin at the level of the fourth lumbar (Fig. 2). Urinary bladder retention was also confirmed. Hematoma and an active bleeding focus were also observed on the right lateral side of the mesorectal area (Fig. 3). Tetanus vaccination and empirical antibiotics were administered, and the patient was then taken to the operating room. A combination of 2 g of cefotetan and 500 mg of metronidazole via intravenous injection was administered.
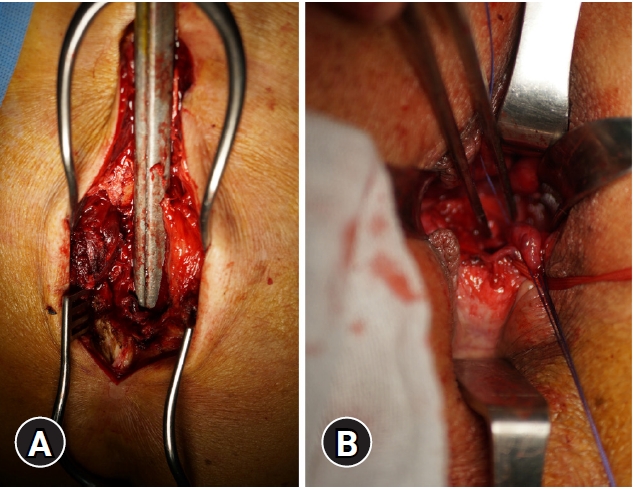
- Our team of neurosurgeons performed an emergency collaborative surgery in combination with the general surgery team. The patient was placed prone on a Wilson table under general anesthesia. The CT scan revealed a bent pipe within the sacral bone, which prevented closed removal. We determined that laminectomy and removal of bony fragments should be the top priority in order to remove the pipe. Routine preparation and drape were performed on the skin and the protruding pipe. A midline skin incision was made from the puncture site of the foreign body to the sacral hiatus. Following dissection of the subcutaneous tissue and muscle, the foreign body and sacrum were exposed (Fig. 4A). We found multiple sacral fractures around the foreign body without cerebrospinal fluid (CSF) leakage. The fractured lamina and bone fragments were removed. Removal of the pipe in one piece increased the risk of bleeding in the visually obscured areas of the penetrating area. Therefore, packing was required for the hematoma and active bleeding focus in the mesorectal area identified in the CT scan. A hole was made using a high-speed drill at the end of the cranial part of the pipe. The hole was connected to a bundle of gauze with a tagging suture. To prevent contamination from bowel contents, the pipe was removed toward the anus by the general surgery team. After removing the foreign body, the tagged bundle of gauze was packed in the mesorectal area. It was confirmed that there was no active bleeding along the packed gauze, and the gauze packed along the trajectory was slowly removed. The pipe was approximately 24 cm long. We observed multiple fractures and injuries to the sacral nerve root from S2 to S4 and the rectum. Right hemilaminectomy of S3, S4, and S5 was performed (Fig. 5). The general surgery team sutured the injured anorectal region through the anus and performed a colostomy (Fig. 4B). No significant bleeding or CSF leakage was detected. The wound was irrigated massively with normal saline. A drain catheter was inserted and the wound was closed layer by layer. There were no specific neurological issues involving motor or sensory function of the lower leg after surgery. The patient was transferred to the intensive care unit after surgery, and the neurological findings remained unchanged and were similar to the patient’s presurgical condition. Sphincter electromyography could not be performed due to the sutured anal wound.
- Antibiotics (500 mg of metronidazole and 2 g of ceftriaxone per day) were administered to the patient intravenously until the 9th day after surgery. The patient’s vital signs were stable without any specific problems on the third day of hospitalization, and the patient was transferred to the general ward. Wound care was terminated, and the patient was discharged on hospital day 13 to a nursing hospital. The Foley catheter was removed 2 weeks after the injury following a consultation with the urology department, and the colostomy required further management. The patient visited the outpatient department on the 22nd day after the injury. Colostomy function was normal without any specific symptoms such as a fever or pain. However, the patient was not able to urinate and had not recovered his anal sphincter tone. The study was approved by the Institutional Review Board of Pusan National University Hospital (No. 2103-008-100). Informed consent for publication of the research details and clinical images was obtained from the patient.
CASE REPORT
- An extensive PubMed search of studies published in the English language found only two cases involving a penetrating injury due to a metallic foreign body piercing through the spine and exiting the body. One similar case involved a penetration injury with a steel rod [3,4]. A PubMed search returned seven cases involving penetrating injuries due to a metallic foreign body stuck in the spine without emerging from the body (Tables 1, 2) [1,3-10]. Although rare, sacral penetrating injuries by foreign bodies, such as nails from nail guns, glass, wood, or metal, have been reported [6]. Likewise, anal penetrating injuries, although uncommon, have also been reported. There were no other cases of a metallic pipe causing a penetrating injury through the anus, rectum, sacrum, and skin. Due to the rarity of this type of injury, there are currently no established guidelines for management or treatment. Therefore, we reviewed similar cases and discussed management strategies below.
- Mechanism of sacral penetrating injuries
- As shown in Table 1, sacral penetrating injuries are mostly caused by falls (nine of 10 cases) [1,3-10]. Such injuries require enough energy to penetrate the body and trigger bone fractures. The trajectory of the foreign object influences whether it completely penetrates the body. If the trajectory is somewhat parallel or oblique to the vertebral body, the velocity of the foreign object will slow down and stop within the bony structures. However, if the angle of the foreign object is approximately perpendicular to the bony structures, the object will exit the body after penetration. Cases illustrating this mechanism are very rare. In order to remove the object without additional injuries, the trajectory should be determined using radiological findings. A foreign object that is bent by the bone like the one found in our case is very difficult to remove and may warrantlaminectomy.
- In the case of a fall-induced penetration injury, the medical professional treating the injury must also evaluate blunt trauma involving other organs during the physical examination and radiological examination. While our case involved an accident sustained due to a fall, there was no blunt trauma involving any body parts other than the area surrounding the trajectory of penetration, possibly due to sufficient deceleration as the foreign object crashed and bent within the bony structure.
- Accompanying injuries
- A patient with a penetrating injury to the torso involving a metallic foreign body should be evaluated for severe trauma [1,11]. The sacrum is located in the pelvis, which contains organs such as the bladder, uterus, vagina, and rectum. It also contains complex vascular structures such as the inferior mesenteric artery, the iliac artery originating from the descending aorta, and the venous plexus. A CT scan must be performed with contrast medium to assess the trajectory of the foreign body and injury to the internal organs, major vessels, bony structures, and active bleeding focus [12]. Eight out of 10 of the cases investigated in the literature review involved sustained concomitant organ damage, and the rectum was the most commonly involved intestinal area. One case involved vaginal damage, and the patient recovered with conservative treatment. Sacral injury can trigger damage to the internal thecal sac and the nerves. Thus, a comprehensive neurological examination is also needed [13]. Nerve injury was observed and laminectomy was performed for nerve decompression in three cases. In one of the cases, nerve anastomosis was also performed. CSF leakage was confirmed in three cases, and death due to sepsis was reported in one case. Repair and spinal fusion operations were staged in two cases. Therefore, if a patient with a sacral penetrating injury presents to the hospital, the accompanying structural damage should be confirmed via a thorough radiological investigation and physical examination. Multidisciplinary treatment is essential and depends on the damaged structure.
- Management and surgical strategy for sacral penetrating injuries
- Management at the site of the accident is very important for patients with injuries that penetrate the body. Paramedics should avoid causing additional damage at the injury site when changing the patient’s body position or removing the foreign body. If the foreign body is too long to be transported, it must be cut to an appropriate length [3]. Such patients should be transported immediately to a hospital with a high-level trauma center where multidisciplinary care is available.
- Before removal of the foreign body, the metallic foreign body must be cut to an appropriate size to avoid additional injury. The two types of cutting tools include scissors and spiral instruments. If a spiral-type cutter is used, cold water should be sprayed to prevent burns to patients caused by the conduction of heat during cutting. This method could also trigger an explosion in the operating room if a mixture of oxygen and nitrous oxide comes in contact with a flame or a high temperature [3]. Penetrating foreign substances must be removed surgically using accurate surgical procedures [1]. If a CT scan confirms an absence of major vessel injuries or active bleeding foci, a closed removal may be attempted. If the foreign body is removed prior to surgery, it is easier to accommodate the patient’s position. In addition, contamination can be avoided using sterilized drapes. If closed removal is impossible, open removal should be performed. Although ensuring an appropriate patient posture can be difficult and there is a risk of contamination, open removal can be controlled with active bleeding, visual confirmation of the involved organs, and immediate spinal canal decompression.
- The purpose of neurosurgical treatment is decompression of the spinal cord, removal of bony fragments and remnants of the foreign body, and the prevention of CSF leakage. Failure to remove any remaining pieces of the foreign body from the penetrated wound may result in CSF leakage, infection, and progressive neurological deficits. If a foreign body is not easily removed due to the bony structures, laminectomy should be performed and bone fragments should be removed to prevent additional injuries to internal organs, blood vessels, and nerves. A fusion operation should also be considered in cases involving severe fractures and a high degree of instability. A fusion operation was performed in three out of 10 the investigated cases, and the procedure was performed in stages according to the risk of infection. Stabilization of the bony structures should be considered in the event of an injury at the level of the lumbo-sacral junction.
- We further analyzed two issues related to treatment for the patient involved in our case. The first issue concerned additional infection by the patient’s bowel contents. We thoroughly performed drape and irrigation of the metallic pipe. In addition, the foreign body was pulled out in the anal direction followed by a colostomy. The second issue was the presence of hematoma and an active bleeding focus on the right lateral side of the mesorectal area identified on the CT scan. Control of the active bleeding was considered a significant challenge because of the narrow and long wound trajectory. Therefore, packing was necessary along the penetrating wound. A hole was made in the upper end of the pipe using a high-speed drill. We connected the hole and the bundle of gauze. The pipe was pulled out in the anal direction along with the gauze, and the penetrated wound was packed with gauze. We successfully treated the injury without causing infection or massive bleeding using the two steps described above.
- Prognosis
- Sacral penetrating injuries are associated with a risk of several complications due to the location of adjacent organs. Tetanus vaccination and appropriate antibiotics should be administered to the patient. In the case of penetration injury by metallic foreign bodies, infection is a major challenge. Sarica et al. [1], who examined several steel rod impalement injuries involving the spine, found that five out of 10 cases were followed by infection. The degree of infection covered a wide spectrum and included wound infection, abscess, sepsis, and death. Penetrating injuries can involve multiple body parts, ranging from the skin to the abdominal cavity, the retroperitoneal cavity, the intestines, and the central nervous system, and broad-spectrum antibiotics should therefore be used. Recommendations for broad-spectrum antibiotics have been explored in another study [14], particularly related to bowel perforation. The specific selection of antibiotics and their uses were different for each reported case. In general, antibiotics to treat skin flora and intestinal bacteria that pass through the blood-brain barrier were selected and administered. A stoma should be placed after a colorectal injury is identified. Eight out of 10 cases involved colorectal injuries, and a stoma was placed to treat patients in each of these cases. Of the 10 patients with sacral penetrating injuries we investigated, three cases resulted in infections, and one of the patients with an infection died due to sepsis.
- In five out of 10 cases, deterioration of the motor and sensory functions was observed in the initial evaluation. One patient died of sepsis, and neurological recovery could not be confirmed. All of the patients underwent laminectomy for decompression. No improvement was detected in two cases, and partial improvement was observed in two cases. Urinary retention as well as an absence of anal tone were observed in the initial evaluation in four out of the 10 cases. The patient subsequently lost the ability to control voiding and defecation in three out of the 10 cases. The patient’s sacral plexus between the S3 and S4 levels was damaged in one recovered case, and the patient underwent laminectomy and reanastomosis. For the patients involved in the remaining three cases and our case, the sacral plexus was severely damaged. This is because the pelvic splanchnic autonomic nerve that runs from the S2 to S4 root regulates bladder and anal functions [15]. In one case, the steel rod penetrated through the sacral bone into the spinal canal at the T12 level, and complete damage occurred to the conus medullaris. In another case, fractures from L4 to S2 after anal penetration led to cauda equina syndrome. Therefore, the degree to which the nerves are affected by a penetration injury should be examined thoroughly, and in addition to sacral plexus injury, conus medullaris syndrome and cauda equina syndrome should also be considered. Therefore, sufficient decompression should be undertaken. Although it was not attempted in most cases, nerve reanastomosis may also be considered.
- Our case involved surgical treatment of a sacral penetrating injury caused by a metallic pipe. More particularly, the reported penetrating injury was through the anus, rectum, sacrum, and lower back. Since sacral penetrating injury is generally accompanied by organ damage due to the anatomical location, a careful examination of accompanying pelvic organ injuries such as rectum and vascular system injuries along with a suitable surgical method are required. In particular, multidisciplinary treatment is recommended to safely remove the foreign body and minimize complications and neurological sequelae.
DISCUSSION
-
Ethical statements
The study was approved by the Institutional Review Board of Pusan National University Hospital (No. 2103-008-100). Informed consent for publication of the research details and clinical images was obtained from the patient.
-
Conflicts of interest
The authors have no conflicts of interest to declare.
-
Funding
None.
-
Author contributions
Conceptualization: IHH; Data curation: MH; Formal analysis: MH; Methodology: IHH, KHN, JHK; Writing–original draft: MH; Writing–review & editing: all authors.
All authors read and approved the final manuscript.
ARTICLE INFORMATION



| Study | Age (yr) | Sex | Mechanism | Kind of foreign body | Entry–exit points | Involved spinal levels | Neurological examination | Accompanying organ damage | Timing of removal |
|---|---|---|---|---|---|---|---|---|---|
| Tokushige et al. (2000) [5] | 66 | Male | Fall | Steel rod | Perianal–none | L5–S1 | Left lower paralysis | Rectum | At the accident site |
| Schildhauer et al. (2005) [6] | 15 | Female | Fall | Steel rod | Perianal–none | S1–5 | Cauda equina syndrome, absent anal tone, perineal sensation | - | NS |
| Serletis et al. (2005) [7] | 6 | Female | Fall | Metallic plant stand | Right buttock–none | S2 | Intact | Vaginal wall, rectum | At the accident site |
| Wang et al. (2009) [8] | 30 | Male | Fall | Steel rod | Right buttock–none | L5–S1 | Intact | Rectum | laparotomy at OR |
| Ritchie et al. (2011) [4] | 28 | Male | In car TA | Metallic pole | Left groin–lower back | S1–2 | Intact | Rectosigmoid | Before laparotomy at OR |
| Zhou et al. (2011) [9] | 37 | Male | Fall | Steel rod | Anus–none | L4-–S2 | Paraparesis, urinary retention, decreased perianal sensation | Rectum | At the accident site |
| Tan et al. (2012) [10] | 32 | Male | Fall | Steel rod | Perineum–none | T12–S1 | T9 paraplegia | Rectum | NS |
| Ozaydın et al. (2018) [3] | 11 | Male | Fall | Steel rod | Anus–lower back | S2–5 | Intact | - | After Laparotomy at OR |
| Sarica et al. (2019) [1] | 37 | Male | Fall | Steel rod | Perineum–none | L4–S1 | Left lower extremity paralysis | Rectum | Before laparotomy at OR |
| This case (2021) | 81 | Male | Fall | Metallic pipe | Anus–lower back | S2–S4 | Urinary retention, absent anal tone | Rectum | After laminectomy at OR |
| Study | Injured nerve | CSF leakage | Operation | Complication | Voiding | Defecation | Outcome |
|---|---|---|---|---|---|---|---|
| Tokushige et al. (2000) [5] | L5 root | Yes | Laparotomy, proctostomy, laminectomy L4, 5, S1 (simultaneous) | Wound infection, presacral abscess, sepsis | NS | NS | Death |
| Schildhauer et al. (2005) [6] | Sacral plexus between S3 and S4 | No | Laparotomy, laminectomy, reduction, S4 root reanastomosis | - | Intact | Intact | Right heel numbness trace weakness of the right plantar flexion |
| Posterior fusion (staged, 3 day) | |||||||
| Serletis et al. (2005) [7] | - | No | Colostomy | - | Intact | Intact | Complete recovery |
| Wang et al. (2009) [8] | - | No | Laparotomy, colostomy | - | Intact | Intact | Complete recovery |
| Ritchie et al. (2011) [4] | - | No | Laparotomy, Hartmann’s procedure | Bowel entrapment | Intact | Intact | Complete recovery |
| Zhou et al. (2011) [9] | - | Yes | Laparotomy, colostomy, laminectomy | Rectal infection, rectal CSF fistula | No control | NS | Improved muscle strength |
| Posterior fusion (staged, 2 mo) | |||||||
| Tan et al. (2012) [10] | - | No | Laparotomy, colostomy, laminectomy (simultaneous) | Epidural abscess, fistula between vertebral canal and rectum | No control | No control | No improvement |
| Ozaydın et al. (2018) [3] | - | No | Laparotomy | - | Intact | Intact | Complete recovery |
| Sarica et al. (2018) [1] | - | Yes | Laparotomy, colostomy, laminectomy | - | Intact | Intact | No improvement |
| Posterior fusion (staged, 14 hr) | |||||||
| Our case (2021) | Sacral plexus S2 | No | Laminectomy, laparotomy, colostomy (simultaneous) | - | No control | No control | No improvement |
- 1. Sarica C, Yucetas SC, Ucler N, et al. Steel rod impalement injuries involving the spine: a case report and literature review. Ulus Travma Acil Cerrahi Derg 2019;25:417–23. ArticlePubMed
- 2. Chen Y, Tang Y, Vogel LC, Devivo MJ. Causes of spinal cord injury. Top Spinal Cord Inj Rehabil 2013;19:1–8. ArticlePubMedPMC
- 3. Ozaydin S, Gulleroglu A, Karaaslan B, et al. Penetrating injury caused by a long iron bar: a case report. North Clin Istanb 2018;5:75–8. ArticlePubMedPMC
- 4. Ritchie ED, Veen EJ, Olsman J, Bosscha K. A case of bowel entrapment after penetrating injury of the pelvis: don't forget the omentumplasty. Scand J Trauma Resusc Emerg Med 2011;19:34. ArticlePubMedPMC
- 5. Tokushige J, Inokuchi A, Kawaguchi H. Impalement injuries involving the spinal canal. J Orthop Sci 2000;5:614–7. ArticlePubMed
- 6. Schildhauer TA, Chapman JR, Mayo KA. Multisegmental open sacral fracture due to impalement: a case report. J Orthop Trauma 2005;19:134–9. ArticlePubMed
- 7. Serletis D, Khoshyomn S, Gerstle JT, Rutka JT. Anterior penetrating sacral injury in a child. Case illustration. J Neurosurg 2005;103(Suppl 5):471. ArticlePubMed
- 8. Wang LT, Wu CC, Hsiao CW, Feng CC, Chang CF, Jao SW. Steel bar penetrating injury of rectum and vertebral body without severe morbidities: report of a case. Dis Colon Rectum 2009;52:346–8. ArticlePubMed
- 9. Zhou Z, Song Y, Cai Q, Li T, Liu H. Penetrating injury of rectum and vertebral body by steel bar causing cauda equina syndrome. Spine (Phila Pa 1976) 2011;36:E803–7. ArticlePubMed
- 10. Tan H, Guo QS, Zhang LY, Sun SJ, Yao YZ, Huang XY. Abscess formation in vertebral canal and presacral area following penetrating injury of rectum and sacral vertebra by a steel rod. Chin J Traumatol 2012;15:241–3. PubMed
- 11. Shahlaie K, Chang DJ, Anderson JT. Nonmissile penetrating spinal injury. Case report and review of the literature. J Neurosurg Spine 2006;4:400–8. ArticlePubMed
- 12. Kim SK, Park YC, Jo YG, Kang WS, Kim JC. Internal iliac artery ligation with pad packing for hemodynamic unstable open comminuted sacral fracture. J Trauma Inj 2017;30:238–41. Article
- 13. Piqueras C, Martinez-Lage JF, Almagro MJ, Ros De San Pedro J, Torres Tortosa P, Herrera A. Cauda equina-penetrating injury in a child. Case report. J Neurosurg 2006;104(Suppl 4):279–81. ArticlePubMed
- 14. Heary RF, Vaccaro AR, Mesa JJ, Balderston RA. Thoracolumbar infections in penetrating injuries to the spine. Orthop Clin North Am 1996;27:69–81. ArticlePubMed
- 15. Chang SM, Hou CL. The frequency and efficacy of differential sacral roots innervation to bladder detrusor in Asian people. Spinal Cord 2000;38:773. ArticlePubMed
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-




- Related articles
-
- Isolated penetrating gluteal stab injury with uncontrolled bleeding in Türkiye: a case report
- Blunt abdominal trauma resulting in pancreatic injury in a pediatric patient in Australia: a case report
- Penetrating gallbladder injury in a pediatric patient: a case report
- Penetrating right ventricular injury following a single gunshot to the left flank in Iraq: a case report
- Experience and successful treatment of craniocerebral gunshot injury at a regional trauma center in Korea: a case report and literature review

