
Articles
- Page Path
- HOME > J Trauma Inj > Volume 36(1); 2023 > Article
-
Original Article
Severity of grinder injuries and related factors compared with other high-rotation cutting tool injuries: a multicenter retrospective study from 2011 to 2018 -
Juni Song, MD1
 , Yang Bin Jeon, MD2, Jae Ho Jang, MD1, Jin Seong Cho, MD1, Jae Yeon Choi, MD1, Woo Sung Choi, MD1
, Yang Bin Jeon, MD2, Jae Ho Jang, MD1, Jin Seong Cho, MD1, Jae Yeon Choi, MD1, Woo Sung Choi, MD1 -
Journal of Trauma and Injury 2023;36(1):32-38.
DOI: https://doi.org/10.20408/jti.2021.0057
Published online: May 25, 2022
- 6,485 Views
- 46 Download
1Department of Emergency Medicine, Gachon Univeristy Gil Medical Center, Gachon University College of Medicine, Incheon, Korea
2Department of Traumatology, Gachon Univeristy Gil Medical Center, Gachon University College of Medicine, Incheon, Korea
- Correspondence to Jae Ho Jang, MD Department of Emergency Medicine, Gachon Univeristy Gil Medical Center, Gachon University College of Medicine, 21 Namdong-daero 774beon-gil, Namdong-gu, Incheon 21565, Korea Tel: +82-32-460-3901 Email: jhjang@gilhospital.com
- Co-correspondence to Yang Bin Jeon, MD Department of Traumatology, Gachon Univeristy Gil Medical Center, Gachon University College of Medicine, 21 Namdong-daero 774beon-gil, Namdong-gu, Incheon 21565, Korea Tel: +82-32-460-3010 Email: junyb@gilhospital.com
Copyright © 2023 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Purpose
- This study aimed to identify the characteristics of patients injured by high-rotation cutting tools and the factors related to the severity of their injuries.
-
Methods
- Adult patients (≥18 years), who presented to the emergency department (ED) after a high-rotation cutting tool injury and who were registered in the Korean Emergency Department-based Injury In-depth Surveillance (2011–2018) database, were included. Patients’ demographic characteristics, injury-related factors, and Injury Severity Scores were collected. All included cases were categorized into two groups according to the tool that caused the injury: grinder versus nongrinder. The characteristics of the two groups were compared, and the factors associated with the severity of injuries were investigated.
-
Results
- Among 8,697 ED visits, 4,603 patients had been using a grinder and 4,094 had been using a nongrinder tool. The most frequently injured body part while using a grinder was the hand (46.4%), followed by the head (23.0%). While using a nongrinder tool, the most frequently injured body part was also the hand (64.0%), followed by the lower leg (11.4%). The odds of a severe injury were affected by patient age (odds ratio [OR], 1.024; 95% confidence interval [CI], 1.020–1.028) and using a grinder (OR, 2.073; 95% CI, 1.877–2.290). The odds of a severe injury using a grinder were higher in arm injuries (OR, 1.60; 95% CI, 1.40–1.83) and multiple-part injuries (OR, 1.998; 95% CI, 1.639–2.437). The odds of a severe injury using a grinder were lower for head injuries (OR, 0.481; 95% CI, 0.297–0.781).
-
Conclusions
- Injuries from grinders were more likely to affect the head and neck than nongrinder injuries, despite the lower severity. The current lack of regulations on grinders in occupational safety and health standards warrants relevant legislation and the development of applicable safety equipment.
- A high-rotation cutting tool is a collective term that refers to machinery used to cut, push, and polish the surface of hard materials such as metal, rocks, or concrete. Many workers present to the emergency department (ED) with injuries from these tools. The number of injuries has increased as the use of grinders has increased in recent years, in part because grinders are compact and easy to use, making them suitable for use as personal tools in the industrial field or at home. While current regulations on industrial safety and health standards mandate the installation of contact prevention equipment on electric saws, such as circular saws and bandsaws, there is a lack of regulation on grinders [1]. Machinery can be easily purchased without meeting specific safety requirements, and there is no legal enforcement of preventive measures such as safety training prior to use, aside from those mandated in workplaces that require training. Furthermore, according to a survey on the workplace environment conducted by the Korean Statistical Information Service, 10.7% of manufacturing workers did not use protective equipment [2].
- Previous studies on grinders focused on case reports involving kickback injuries to the head and neck regions. A kickback injury occurs when a rapidly rotating saw blade catches on material that is not firmly fastened and that the blade is unable to cut through, causing the material to twist and launch (or “kick”) back from the blade at high speed 8. A study of 133 participants demonstrated the frequency of facial damage caused by high-rotation cutting tools such as grinders (62%), chainsaws (32%), and rotary saws (15%) [3,4]. Based on these results, this study aimed to determine the relative risk of grinders compared to other high-rotation cutting tools by investigating patients who had visited the ED in the past few years. In particular, the study focused on head and neck injuries sustained from high-rotation cutting tools.
INTRODUCTION
- The study was approved by the Institutional Review Board of Gachon University Gil Medical Center (No. GBIRB2021-202). The need for informed consent was exempted due to the retrospective nature of the study. This retrospective study used data from the Korean Emergency Department-based Injury In-depth Surveillance (EDIIS) conducted as part of the hospital injury monitoring system of the Korea Disease Control and Prevention Agency [5].
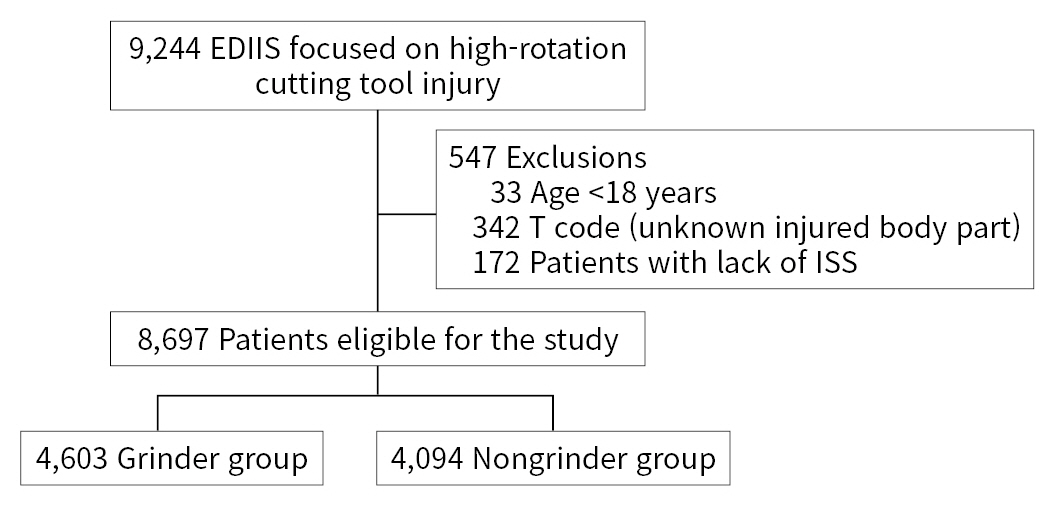
- The study analyzed patients who presented to the participating ED between January 2011 and December 2018 and were evaluated for suspected injuries from manually operated high-rotation cutting tools, such as electric chainsaws and grinders. Of the 9,244 individuals whose data were collected, 33 who were under 18 years of age, 342 with an unspecified area of injury, and 172 with missing data on the severity of the injury were excluded. In total, 8,697 participants were included in the final analysis (Fig. 1).
- Participants were divided into two groups: patients who sustained injuries from grinders and those injured by tools other than grinders. The general characteristics of the participants were collected, including age, sex, means of transportation to the hospital, place of injury, activity during injury, time of injury, diagnostic results, and whether surgery was performed. The place of injury was divided into industrial workplace, home, and miscellaneous, while the activity at the time of injury was divided into working, nonworking, and miscellaneous. Considering different work shifts, time of injury was divided into four time periods: morning (06:00–11:59), afternoon (12:00–17:59), evening (18:00–23:59), and night (00:00–05:59). The ED outcomes were divided into discharge, transfer, admission to the general ward, admission to the intensive care unit (ICU), death, and miscellaneous. Subgroups were created within transfers based on the following: lack of rooms in the general ward, lack of rooms in the ICU, inability to provide immediate emergency surgery or care, transfer to tertiary hospitals for specialized emergency care, transfer to primary and secondary medical institutions because severity of the injury was low, transfer to specialized long-term care facilities, personal requests, and miscellaneous. Up to 10 diagnoses were investigated per patient, with each assigned to one of 10 categories based on the location of the injury: head, neck, thorax, abdomen, upper arm, lower arm, hand, upper leg, lower leg, and foot; with the addition of four subgroups of areas (the head and neck, torso, upper limb, and lower limb) for comparison.
- The Excessive Mortality Ratio-adjusted Injury Severity Score (EMR-ISS) uses the S and T codes from the International Classification of Disease (ICD), and after rating the severity of each diagnosis on a scale of 1 to 5, the three highest-scoring codes, regardless of the area of injury, are taken, squared, and then added to produce a final score [6]. Major or severe trauma is most often defined as a score of ≥16 when assessing severity. For the purposes of this study, EMR-ISS scores of 1 to 8 were defined as mild trauma, 9 to 15 as moderate trauma, and ≥16 as severe trauma [7,8]. Additional divisions of EMR-ISS scores (1–8 and ≥9) were added to enable multivariate analysis of the severity of injury. Calculating the Injury Severity Score (ISS) requires a detailed assessment of the injury. There are many items that must be carefully evaluated by a specialized assessor. This study collected data based on the EDIIS guidelines. The data were collected by an emergency responder, not a clinician, who interviewed the patient, and the EMR-ISS inevitably used the emergency room diagnosis because evaluation data after hospitalization were not available. The EMR-ISS is basically derived from the ICD, as is the ICD-derived Injury Severity Score (ICISS). However, these systems calculate specific values differently and, according to previous studies, the EMR-ISS demonstrated better calibration and discrimination power for prediction of death than the ICISS in most injury groups [6]. This study presented severity by utilizing the EMR-ISS national data, as collected by the Korea Disease Control and Prevention Agency.
- For statistical analysis, the nominal variables of descriptive data were described in numbers and percentages and univariate analysis was performed using the chi-square test. Multivariate logistic regression analysis was used to compare severity, with the variables that showed a P-value <0.1 in the univariate analysis as input variables. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated and P<0.05 was used as the threshold for statistical significance. Statistical analysis was performed using IBM SPSS ver. 24.0 (IBM Corp., Armonk, NY, USA).
METHODS
- General characteristics and location of injury in patients injured by high-rotation cutting tools
- As shown in Tables 1 and 2, a total of 8,697 participants were included in this study. Injuries from high-rotation cutting tools occurred more often in male patients for both categories of injuries (grinder injuries, 4,523 [98.3%]; nongrinder injuries, 3,955 [96.6%]) than in female patients (grinder injuries, 80 [1.7%]; nongrinder injuries, 139 [3.4%]). In the grinder group, 1,502 injuries (32.6%) occurred in the morning, 2,360 (51.3%) in the afternoon, 635 (13.8%) in the evening, and 106 (2.3%) at night. In the nongrinder group, 1,319 injuries (32.2%) occurred in the morning, 2,183 (53.3%) in the afternoon, 489 (11.9%) in the evening, and 103 (2.5%) at night. The number of patients injured during work was 3,920 (85.2%) in the grinder group and 3,229 (78.9%) in the nongrinder group, with the rest having occurred in activities outside of work. Similarly, the number of injuries at industrial workplaces was 3,553 (77.2%) in the grinder group and 2,575 (62.9%) in the nongrinder group. The most frequently injured body parts in the grinder group were 2,136 hands (46.4%), 1,059 heads (23.0%), 545 lower legs (11.8%), and 453 lower arms (9.8%). Concurrently, the nongrinder group had injuries to 2,623 hands (64.0%), 466 lower legs (11.4%), 419 heads (10.2%), and 291 lower arms (7.1%). Assessment of the distribution of injuries according to the four higher-level divisions showed that the grinder group had 1,113 injuries (24.2%) in the head and neck, 117 (92.5%) in the torso, 2,625 (57.0%) in the upper limbs, and 895 (19.4%) in the lower limbs, while the nongrinder group had 454 injuries (11.0%) in the head and neck, 61 (1.5%) in the torso, 2,908 (71.0%) in the upper limbs, and 740 (18.1%) in the lower limbs. Isolated injuries (i.e., injuries focused in only one of the four divisions) totaled 3,657 (79.4%) in the grinder group and 3,251 (79.4%) in the nongrinder group, while multiple injuries (affecting two or more parts) totaled 946 (20.6%) in the grinder group and 843 (20.6%) in the nongrinder group. Among the patients with available surgical records, 14.4% of the grinder group and 17.5% of the nongrinder group underwent surgery. The outcomes in the grinder group were 3,196 discharge (69.4%), 968 admission to the general ward (21.0%), and 408 transfer (8.9%). The outcomes in the nongrinder group similarly included 3,229 discharge (56.0%), admission to the 1,196 general ward (29.2%), and 564 transfer (13.8%). In the grinder group, mild trauma was found in 2,995 patients (65.1%), moderate trauma in 1,512 (32.8%), and severe trauma in 96 (2.1%). Meanwhile, in the nongrinder group, mild trauma was found in 3,186 patients (77.8%), moderate trauma in 817 (20.0%), and severe trauma in 91 (2.2%). The average age was 50.0 years old in the grinder group and 52.7 years old in the nongrinder group.
- Univariate analysis was conducted to compare the severity of injury between the two groups based on EMR-ISS scores: <9, mild severity; and ≥9, moderate to severe severity. Age, sex, activity during the injury, place of injury, and use of grinders were used to analyze the collected variables. The results indicated differences in severity depending on age, sex, activity during injury, and usage of a grinder.
- Risk factors associated with EMR-ISS scores
- As presented in Table 3, the risk for a severe injury (using an EMR-ISS score of 9 as the standard) was compared using logistic regression analysis. Sex, age, grinder usage, and activity during the injury were analyzed. In all patients, higher risk was associated with multiple injuries (two or more injured body parts), older age (OR, 1.027; 95% CI, 1.018–1.036) and grinder usage (OR, 1.998; 95% CI, 1.639–2.437). In patients with head and neck injuries, the risk increased with age (OR, 1.027; 95% CI, 1.012–1.043) but decreased with grinder usage (OR, 0.481; 95% CI, 0.297–0.781). The risk of a severe torso injury increased with age (OR, 1.096; 95% CI, 1.023–1.176). Patients with arm injuries had an increased risk of a severe injury with age (OR, 1.015; 95% CI, 1.004–1.027) and grinder use (OR, 1.60; 95% CI, 1.40–1.83). In patients with leg injuries, a lower risk for a severe injury was found if the injury occurred during work (OR, 0.481; 95% CI, 0.297–0.781).
RESULTS
- This study aimed to provide a foundation for the establishment of injury prevention strategies by conducting an analysis of patients with injuries sustained from high-rotation cutting tools. Previous international studies on injuries caused by grinders have been limited to case studies focusing on head and neck injuries alone [9]. They described the characteristics of the tools causing the injury (type, size and rotation speed of the saw blade, facial area hit by the blade, and the distance between the patient and machine) and emphasized the need to prevent injuries through education on proper usage of the tools [10]. Other case studies illustrated the management and treatment of injuries resulting from the use of angle grinders [11]. The objective risks associated with grinders have not been statistically measured due to the lack of statistical data and the limitations of measuring severe injuries. Therefore, previous studies did not deal with the relative risk of the grinder, but simply described its safe use and the treatment of grinder injuries.
- Among the limited number of previous Korean studies, a case report on disorders of peripheral blood vessels and the peripheral nervous system of the hands and fingers caused by the use of vibrating tools such as grinders was published in the Journal of the Korean Society of Occupational and Environmental Medicine [12]. Another study by the Korean Society of Manufacturing Process Engineers investigated grinder tools capable of angle adjustment [13]. Thus, our current study emphasized the significance of evaluating the risks associated with the use of high-rotation cutting tools in Korea.
- There was a higher occurrence of head injuries in the grinder group than in the nongrinder group, likely due to head injuries resulting from kickback by grinders. Grinders are prone to produce more kickback than other high-rotation cutting tools. To date, research has been conducted on the safety features of other high-rotation cutting tools such as rotary saws or chainsaws (e.g., saw stops that program machines to stop upon detection of conductive materials such as fingers near the vicinity of the saw blade); however, no protective function has been applied to grinders. Despite reported incidents, the lack of legal mandates on safety equipment for grinders, such as protective covers that reduce kickback, is concerning. In contrast, regulations have been placed on other high-rotation cutting tools, consequently contributing to the higher incidence of kickback injuries in grinder use. Nonetheless, regulations on grinders are still overlooked in occupational safety and health standards.
- Risk increased with age in patients with multiple injuries (i.e., in more than two areas), as well as for patients with torso or arm injuries. While previous research has attributed a decrease in workplace performance to decreasing physical abilities [14,15], this study found the difference in risk related to age was small and statistically insignificant.
- Despite the initial assumption that a higher proportion of head and neck injuries in the grinder group would indicate higher severity than in the nongrinder group, the former had less severe head and neck injuries. The higher number of head and neck injuries observed in the grinder group raises concerns about survival bias. Severe head and neck injuries often result in death at the scene before the patient can be transported to the ED and resuscitated, despite the prehospital communication between rescue services personnel and the medical team. This would result in patients with injuries severe enough to cause death being excluded from the EDIIS, which would lower the severity of injuries in the grinder group. It is also possible that the severity could be lowered during the EMR-ISS scoring process. Head and neck injuries are not given higher severity scores than other injuries in the EMR-ISS, as the scale does not incorporate the area of injury in its assessment and depends solely on the severity of the injury itself: 1, minor injury; 2, moderate injury; 3, serious injury; 4, severe injury; 5, critical injury; and 6, maximal/untreatable injury. The EMR-ISS also has a limited ability to evaluate the severity of puncture wounds which can be caused by kickback injuries [8]. A final possibility is that grinder injuries may indeed have lower severity because grinders are powered by batteries rather than the high voltage alternating current used by other high-rotation cutting tools, resulting in a comparatively lower cutting speed and strength.
- There were several limitations to this study. First, the data used were collected from only 23 hospitals, not from all institutions in Korea, making it difficult to generalize the results as representative of all Korean patients injured by high-rotation cutting tools. Second, there was potential for sampling bias in the comparison of grinder and nongrinder groups, since the use of protective equipment that lowered the likelihood of injuries produced a unique personal characteristic that was not accounted for in this study. Third, the retrospective design prevented the analysis of data missing from the EDIIS. In particular, there were missing data on protective equipment (because it was optional) and on whether the safety and health training for the use of the tool was completed. Another limitation was the possible removal of a part of the diagnostic T-code that represents injuries to unspecified body parts, causing errors in the total number of multiple injuries. Fourth, it was not possible to objectively account for the risk associated with each tool, making it difficult to compare injury severity with usage risk, which would have been useful in analyzing the high frequency and low severity observed for head and neck injuries in the grinder group. Finally, a limitation of the EMR-ISS is that it lacks an appropriate stratification for injuries in the same body part. For example, even if two or more injuries occur in the same area of the body, there is a problem that only one injury is applied to the severity calculation. In severe trauma cases, the EMR-ISS does not measure the severity of injury as well as the ISS, which can evaluate the depth of injury, the extent of injury, and the functional deficits resulting from the injury. However, in this study, there were few patients who could be classified as having severe trauma, so we would expect little difference in our results if the ISS had been used for evaluation. In the case of grinders and rotary cutting tools, most of the injuries that would have been considered as severe trauma were likely to have caused death at the scene of an accident or during transport.
- In conclusion, injuries from grinders were more likely to affect the head and neck than nongrinder injuries, despite their lower severity. The current lack of regulations on grinders in occupational safety and health standards warrants relevant legislation and the development of applicable safety equipment.
DISCUSSION
-
Ethical statements
The study was approved by the Institutional Review Board of Gachon University Gil Medical Center (No. GBIRB2021-202). The need for informed consent was exempted due to the retrospective nature of the study.
-
Conflicts of interest
The authors have no conflicts of interest to declare.
-
Funding
None.
-
Author contributions
Conceptualization: YBJ, JHJ; Methodology: JS, YBJ, JHJ, JSC; Data curation: JSC, JYC; Formal analysis: JSC, JYC, JHJ; Writing–original draft: JS, JHJ; Writing–review&editing: WSC, JSC, YBJ, JHJ, JYC. All authors read and approved the final manuscript.
ARTICLE INFORMATION
| Characteristic | No. of patients | P-value | |
|---|---|---|---|
| Grinder (n=4,603) | Nongrinder (n=4,094) | ||
| Body parta) | <0.05 | ||
| Head | 1,059 (23.0) | 419 (10.2) | |
| Neck | 65 (1.4) | 48 (1.2) | |
| Chest | 41 (0.9) | 33 (0.8) | |
| Abdomen | 76 (1.7) | 33 (0.8) | |
| Upper arm | 92 (2.0) | 59 (1.4) | |
| Lower arm | 453 (9.8) | 291 (7.1) | |
| Hand | 2,136 (46.4) | 2,623 (64.0) | |
| Upper leg | 168 (3.6) | 117 (2.9) | |
| Lower leg | 545 (11.8) | 466 (11.4) | |
| Foot | 209 (4.5) | 173 (4.2) | |
| Four parts of body | <0.05 | ||
| Head and neck | 1,113 (24.2) | 454 (11.0) | |
| Torso | 117 (2.5) | 61 (1.5) | |
| Upper limb | 2,625 (57.0) | 2,908 (71.0) | |
| Lower limb | 895 (19.4) | 740 (18.1) | |
| Damaged parts | <0.05 | ||
| Single part | 3,657 (79.4) | 3,251 (79.4) | |
| Multiple parts | 946 (20.6) | 843 (20.6) | |
- 1. Ministry of Employment and Labor. Enforcement Decree of the Occupational Safety and Health Act [Internet]. Korean Law Information Center; 2021 [cited 2021 Jul 1]. Available from: https://www.law.go.kr/LSW/eng/engLsSc.do?menuId=2&query=ENFORCEMENT%20DECREE%20OF%20THE%20OCCUPATIONAL%20SAFETY%20AND%20HEALTH%20ACT#liBgcolor0.
- 2. Korean Statistical Information Service (KOSIS). Personal protection equipment wearing rate [Internet]. KOSIS; 2021 [cited 2021 Jul 1]. Available from: https://kosis.kr/statHtml/statHtml.do?orgId=380&tblId=DT_380002_D004A&conn_path=I2.
- 3. Konstantinovic VS, Puzovic D, Anicic B, Jelovac DB. Epidemiological, clinical, and forensic aspects of chainsaw, circular saw, and grinding saw injuries in the maxillofacial region. J Craniofac Surg 2010;21:1029–32. ArticlePubMed
- 4. Marks RB, Fort F. Chain saw injury of the maxillofacial region. J Oral Maxillofac Surg 1986;44:240–3. ArticlePubMed
- 5. Korea Disease Control and Prevention Agency (KDCA). 2018 In-depth investigation guide for injured patients [Internet]. KDCA; 2019 [updated 2021 Sep 2; cited 2021 Jul 1]. Available from: https://www.kdca.go.kr/injury/biz/injury/recsroom/examinGudbkMain.do.
- 6. Kim J, Shin SD, Im TH, et al. Development and validation of the excess mortality ratio-adjusted Injury Severity Score using the International Classification of Diseases 10th edition. Acad Emerg Med 2009;16:454–64. ArticlePubMed
- 7. Palmer C. Major trauma and the injury severity score: where should we set the bar? Annu Proc Assoc Adv Automot Med 2007;51:13–29. PubMedPMC
- 8. Jung K, Lee CJ, Kim J. Injury Severity Scoring system for trauma patients and trauma outcomes research in Korea. J Acute Care Surg 2016;6:11–7. Article
- 9. Koehler SA, Luckasevic TM, Rozin L, et al. Death by chainsaw: fatal kickback injuries to the neck. J Forensic Sci 2004;49:345–50. ArticlePubMed
- 10. Vosbikian MM, Harper CM, Byers A, Gutman A, Novack V, Iorio ML. The impact of safety regulations on the incidence of upper-extremity power saw injuries in the United States. J Hand Surg Am 2017;42:296. Article
- 11. Khurram SA, Atkins S, Smith KG, Yates JM. A multidisciplinary approach to management of extensive facial injuries resulting from the use of an angle grinder. Injury Extra 2011;42:75–8. Article
- 12. Yim SH, Kim RH, Yang GS, et al. 6 Cases of hand arm vibration syndrome in grinding workers exposed to hand-arm vibration. Korean J of Occup Environ Med 2000;12:421–9. ArticlePDF
- 13. Oh B, Choi MK, Park JW, Kim JH, Woo SJ, Son IS. Angle-adjustable grinder tool unit. Proceedings of the Spring/Autumn Conference of the Korean Society of Manufacturing Process Engineers; 2017 Oct 19; Gongju, Korea.
- 14. Baltes PB, Lindenberger U. Emergence of a powerful connection between sensory and cognitive functions across the adult life span: a new window to the study of cognitive aging? Psychol Aging 1997;12:12–21. ArticlePubMed
- 15. Wagner-Hartl V, Grossi NR, Kallus KW. Impact of age and hearing impairment on work performance during long working hours. Int J Environ Res Public Health 2018;15:98. ArticlePubMedPMC
 PubReader
PubReader ePub Link
ePub Link Cite
Cite

