Sphenoid sinus foreign body following airbag deployment in the United States: a case report
Article information

Abstract
We report a unique case of penetrating foreign bodies following a motor vehicle accident with airbag deployment. The patient presented with evidence of facial trauma and was found to have three retained foreign bodies on imaging. Notably, one foreign body was within the sphenoid sinus. This foreign body was removed uneventfully through endoscopic sinus surgery. The patient was doing well at follow-up visits. We concluded that the foreign bodies were steering wheel accessories, which detached upon airbag deployment and penetrated the patient’s face. This case report is intended to inform the public regarding the dangers of placing accessories on a steering wheel.
INTRODUCTION
Sinonasal foreign bodies are rare, but concerning due to nearby critical structures, including the orbit, optic nerves, internal carotid arteries, brain, and cavernous sinus. Due to the proximity of these structures, sinonasal foreign bodies can result in significant complications. Within the orbit, traumatic foreign body injury can result in visual disturbance, diplopia, ophthalmoplegia, or infectious complications, whereas sinonasal complications may include nasal obstruction, sinusitis, smell disturbance, cerebrospinal fluid rhinorrhea, life-threatening hemorrhage, or stroke.
Several traumatic cases of traumatic sinonasal foreign bodies have been reported. Most commonly, injuries involving high-velocity trauma, such as firearms [1–3], ballistic projectiles [4], and high falls [5,6], increase the risk of penetrating foreign bodies. However, even falls from standing height impart enough force to result in sinus penetration [7,8]. Foreign body entry wounds frequently involve the nasal cavity [2,3,5,8] and orbit [1,6,7]. These foreign bodies are typically less than a centimeter in all dimensions. For cylindrical objects, at least one two-dimensional face of less than 1 cm2 is typical, such as a wooden stick [6,8] or pen [5]. We report a case of a sphenoid sinus foreign body resulting from airbag deployment during a motor vehicle accident (MVA).
CASE REPORT
The patient was a 31-year-old woman without any relevant medical history brought to our emergency department following a head-on MVA with airbag deployment. She was alert and only complained of pain along her lower face and minor epistaxis. Her only obvious injuries were two small puncture wounds over her chin and right mandible. Due to the nature of the accident, a full-body computed tomography scan was obtained, which demonstrated metallic densities within the facial soft tissues and within the right posterior ethmoid and sphenoid sinus, abutting the paraclival carotid artery (Fig. 1). The appearance of the foreign body on imaging was similar to what would be expected from a screw. Given the proximity of the foreign body to the carotid artery a computed tomography angiogram was obtained that did not identify any major vascular injury (Fig. 2).
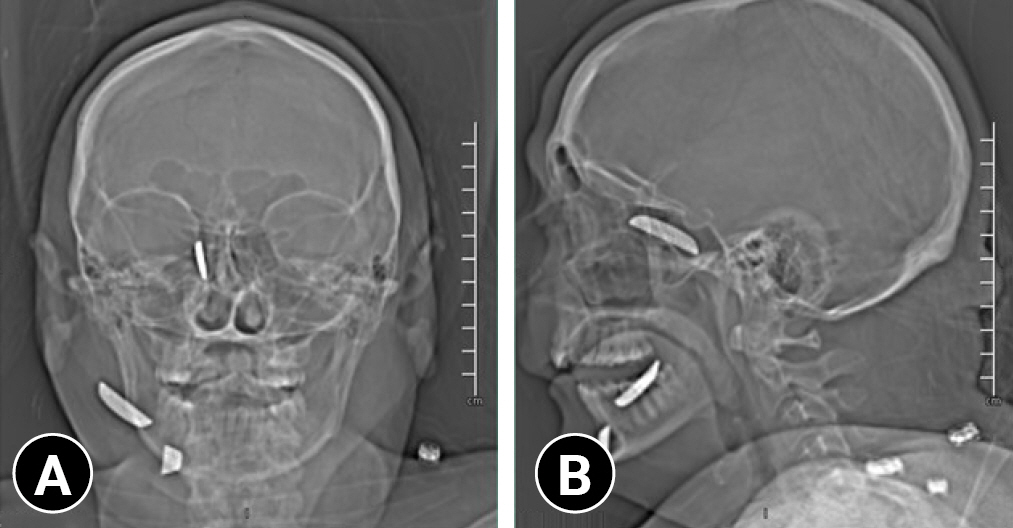
Scout x-ray showing location of foreign bodies. (A) Anteroposterior and (B) lateral X-ray demonstrating the location of the foreign bodies in the facial soft tissue and right sphenoid sinus.
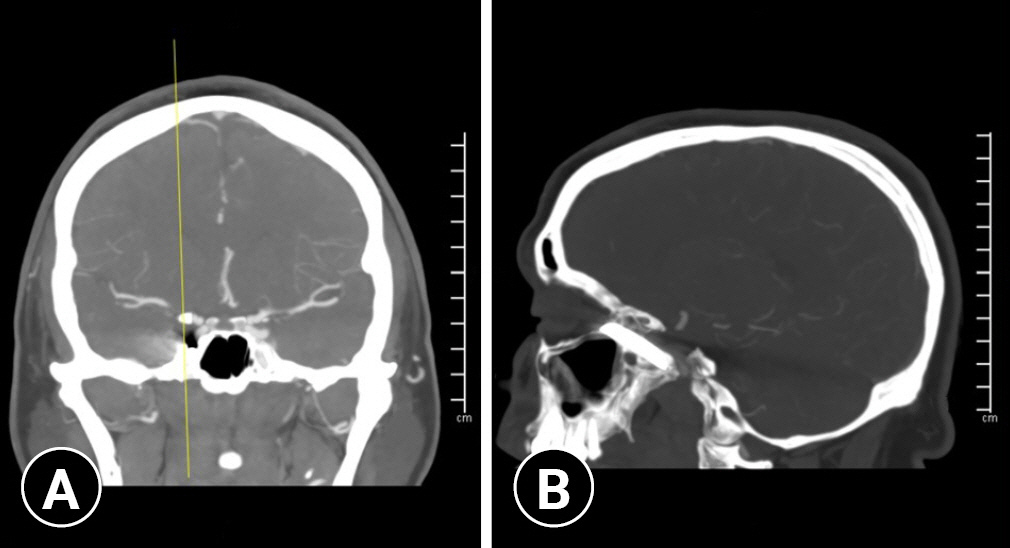
Coronal and sagittal images from a computed tomography angiogram. (A) Coronal image showing the location of the foreign body in lateral sphenoid sinus (yellow line) and proximity to the cavernous carotid artery. (B) Sagittal image showing the proximity of the foreign body to the cavernous carotid artery.
In preparation for endoscopic removal of the foreign body, the neurointerventional radiology team was consulted in the unlikely event of an unexpected injury to the carotid artery. Interestingly, it was recognized that the foreign body had entered through the left nasal cavity, traversed the head of the left inferior turbinate, penetrated through the septum, and entered the right posterior ethmoid and sphenoid sinus (Figs. 3, 4). The approach began with resection of the right middle turbinate, which would give wide access to the sphenoid in the event of excessive bleeding. A standard maxillary antrostomy and ethmoidectomy were then performed. The sphenoid sinus was then entered along its medial aspect to avoid any manipulation of the foreign body. Careful lateral dissection then exposed the distal aspect of the foreign body lodged in the clival recess of the sphenoid sinus. The proximal aspect of the foreign body was then exposed along the lamina papyracea after some edematous mucosa was removed. The foreign body was then removed with Takahashi forceps without any adverse event. No skull base injury or major neurovascular injury was encountered during the approach or removal.
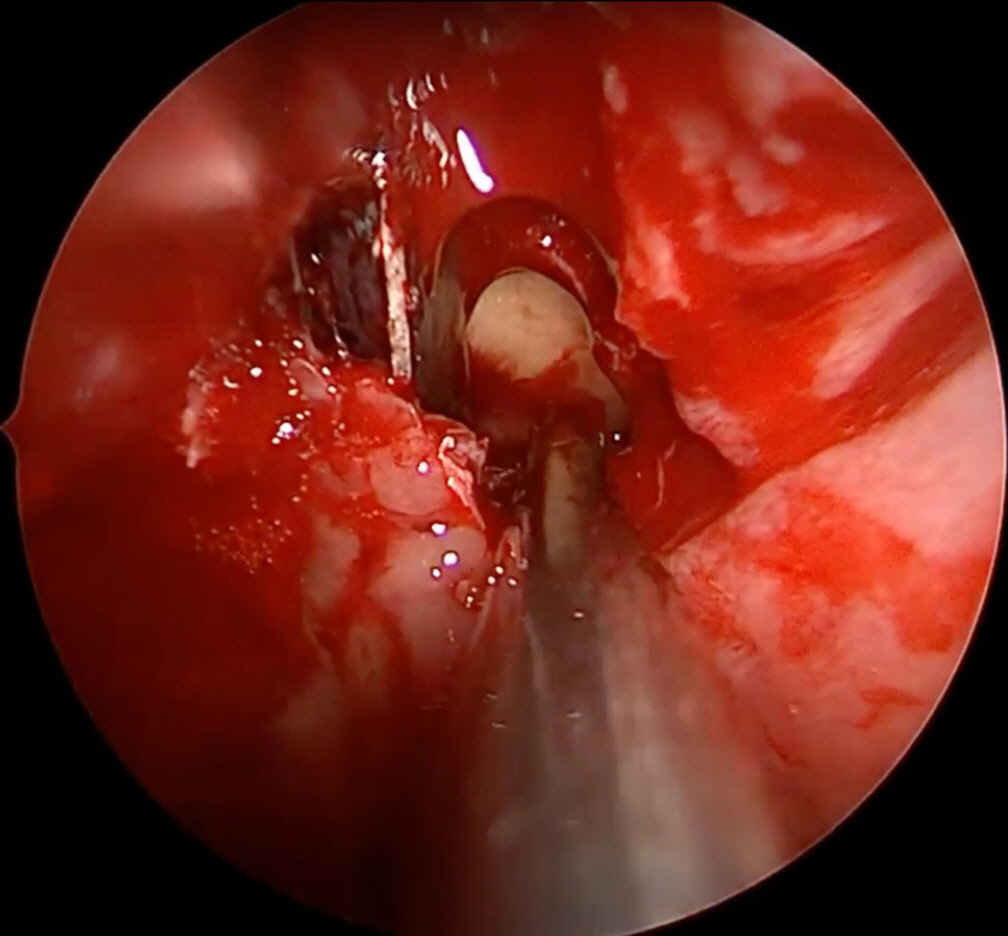
Intraoperative view of the foreign body projecting inferiorly within the lateral aspect of the right sphenoid sinus.

Foreign bodies following removal.
At the patient’s latest follow-up, 1 month after surgery, she had some synechiae in the left nasal cavity, which were lysed. This was in the area where the foreign body penetrated the septum. Otherwise, she had resolving edema of the maxillary sinus, but had no long-lasting effects from the injury.
Ethics statements
Written informed consent for publication of the research details and clinical images was obtained from the patient.
DISCUSSION
MVAs are the most common cause of serious facial trauma [9]. Standard safety features, such as seatbelts and airbags, significantly reduce facial trauma [10], but have limitations at high speeds [11] and are associated with their own injuries. Injuries related to airbag deployment mostly affect the face (42%), with minor burns and abrasions being typical [12]. Serious cases of penetrating injury attributed to airbag deployment have been reported [13,14], and in the past decade, several automobile fatalities were directly attributed to defective airbags.
In November 2014, the US National Highway Traffic Safety Administration ordered a nationwide recall of Takata airbags, affecting 34 million vehicles on US roads, the largest automobile recall in history. The recalled airbags contained a defective inflator, which resulted in either slow airbag deployment or, more dangerously, explosion of the inflator. To date in the United States, 19 deaths have been attributed to these airbags, including 16 in Honda vehicles (Los Angeles, American Honda Motor) according to the Honda company website [15].
The patient in this case was driving a Honda, and had affixed aftermarket accessories to her steering wheel, as pictured in Fig. 5. Whether a defective airbag contributed to her facial injuries is unknown; however, the most likely explanation of her facial injuries is dislodgement of steering wheel accessories during airbag deployment, creating projectiles near the patient’s face. Entry through the nasal cavity and ultimate embedment in the sphenoid sinus is highly suggestive of a direct course starting near the steering wheel and demonstrates the force with which airbags deploy. The trajectory of the foreign body through the patient’s septum and its terminus within the sphenoid sinus adjacent to critical neurovascular structures makes this case a fortunate close call.

Foreign bodies arranged within the Honda logo.
In our review of the scientific literature, we found no similar reported cases of injury by steering wheel accessories. However, there has been speculation regarding the dangers of these objects in the lay media. This is based on the logical concern regarding a loosely adhered object over an airbag, which is designed to explode violently. As of this report, these products are widely available to consumers without an associated safety warning. The goal of this report is to bring awareness to the potential danger posed by steering wheel accessories in the event of airbag deployment.
While penetrating sinonasal foreign bodies are rare entities within the trauma community, it is important to keep in mind that they may occur even in the absence of obvious entry wounds. Additionally, consumers should beware that placement of aftermarket products over airbags may turn these benign objects into dangerous projectiles upon airbag deployment.
Notes
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
None.
Data sharing statement
Not applicable.
Author contributions
Conceptualization: all authors; Data curation: all authors; Formal analysis: all authors; Methodology: all authors; Project administration: all authors; Visualization: all authors; Writing–original draft: all authors; Writing–review & editing: all authors. All authors read and approved the final manuscript.