Articles
- Page Path
- HOME > J Trauma Inj > Volume 36(3); 2023 > Article
-
Original Article
Factors associated with the injury severity of falls from a similar height and features of the injury site in Korea: a retrospective study -
Dae Hyun Kim, MD1
 , Jae-Hyug Woo, MD1*, Yang Bin Jeon, MD2*, Jin-Seong Cho, MD1, Jae Ho Jang, MD1, Jea Yeon Choi, MD1, Woo Sung Choi, MD1
, Jae-Hyug Woo, MD1*, Yang Bin Jeon, MD2*, Jin-Seong Cho, MD1, Jae Ho Jang, MD1, Jea Yeon Choi, MD1, Woo Sung Choi, MD1 -
Journal of Trauma and Injury 2023;36(3):187-195.
DOI: https://doi.org/10.20408/jti.2022.0042
Published online: November 16, 2022
- 1,611 Views
- 59 Download
1Department of Emergency and Critical Care Medicine, Gachon University Gil Medical Center, Gachon University College of Medicine, Incheon, Korea
2Department of Traumatology, Gachon University Gil Medical Center, Gachon University College of Medicine, Incheon, Korea
- Correspondence to Jae-Hyug Woo, MD Department of Emergency and Critical Care Medicine, Gachon University Gil Medical Center, Gachon University College of Medicine, 21 Namdong-daero 774beon-gil, Namdong-gu, Incheon 21565, Korea Tel: +82-32-460-3901 E-mail: emmetalkiller@gilhospital.com
- Yang Bin Jeon, MD Department of Traumatology, Gachon University Gil Medical Center, Gachon University College of Medicine, 21 Namdong-daero 774beon-gil, Namdong-gu, Incheon 21565, Korea Tel: +82-32-460-3010 E-mail: junyb@gilhospital.com
- *Jae-Hyug Woo and Yang Bin Jeon contributed equally to this work.
Copyright © 2023 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Purpose
- This study aimed to determine the risk factors associated with the severity of fall-related injuries among patients who suffered a fall from similar heights and analyze differences in injury sites according to intentionality and injury severity.
-
Methods
- The Emergency Department-based Injury In-depth Surveillance (EDIIS) data collected between 2019 and 2020 were used in this retrospective study. Patients with fall-related injuries who fell from a height of ≥6 and <9 m were included. Patients were categorized into the severe and mild/moderate groups according to their excessive mortality ratio-adjusted Injury Severity Score (EMR-ISS) and the intention and non-intention groups. Injury-related and outcome-related factors were compared between the groups.
-
Results
- In total, 33,046 patients sustained fall-related injuries. Among them, 543 were enrolled for analysis. A total of 256 and 287 patients were included in the severe and mild/moderate groups, respectively, and 93 and 450 patients were included in the intention and non-intention groups, respectively. The median age was 50 years (range, 39–60 years) and 45 years (range, 27–56 years) in the severe and mild/moderate groups, respectively (P<0.001). In multivariable analysis, higher height (odds ratio [OR] 1.638; 95% confidence interval [Cl], 1.279–2.098) and accompanying foot injury (OR, 0.466; 95% CI, 0.263–0.828) were independently associated with injury severity (EMR-ISS ≥25) and intentionality of fall (OR, 0.722; 95% CI, 0.418–1.248) was not associated with injury severity. The incidence of forearm injuries was four (4.3%) and 58 cases (12.9%, P=0.018) and that of foot injuries was 20 (21.5%) and 54 cases (12.0%, P=0.015) in the intention versus non-intention groups, respectively.
-
Conclusions
- Among patients who fell from a similar height, age, and fall height were associated with severe fall-related injuries. Intentionality was not related to injury severity, and patients with foot injury were less likely to experience serious injuries. Injuries in the lower and upper extremities were more common in intentional and unintentional falls, respectively.
- Background
- In Korea, slips and falls are the most common causes of injuries among patients presenting to the emergency department (ED). In 2020, 68,904 patients suffered from slips and falls, representing 33.3% of patients presenting to the ED. Among patients with injuries due to slips and falls, approximately 21% suffer fall-related injuries and present to the ED [1]. Hospitalization and mortality rates are higher among the patients who suffer a fall than among patients with other injuries. Additionally, several patients who suffer a fall also suffer from disability after discharge, which leads to difficulties in returning to daily life and work. Clinicians in EDs or trauma centers also experience difficulties in treating patients who suffer a fall, as they often present with severe injuries and multiple traumas.
- Several studies have investigated the risk factors associated with the severity of fall-related injuries. Known risk factors include the fall height and the age and body mass index of the patient [2–5]. Additionally, intentional falls are associated with more severe injuries than unintentional falls [6,7]. However, the aforementioned studies reported that the mean fall height was greater in intentional falls than in unintentional falls; as such, differences in the severity of injuries between intentional and unintentional falls may be attributed to the simple difference in fall height. Furthermore, studies have reported differences in the injury site. Intentional falls tend to result in a higher frequency of injuries in the lower extremity, whereas unintentional falls are more commonly associated with head injuries [7]. Several studies have also reported the differences in injury site depending on the fall height [8,9]. At present, it is unclear whether the differences in injury site between intentional and unintentional falls are due to the intention of the patients.
- Fall height has a significant effect on the clinical outcome of patients with fall-related injuries [10,11]. Therefore, the independent effects of other risk factors may be masked by the effects of fall height. To elucidate the effects of other risk factors, it may be helpful to compare the clinical features of the patients who suffer fall-related injuries after falling from similar heights.
- Objectives
- This retrospective study aimed to investigate the patients with fall-related injuries from a similar fall height, who were divided into severe and nonsevere cases to identify risk factors related to the severity of injury, and examine the differences in patient characteristics and injury site between intentional and unintentional falls from a similar fall height.
INTRODUCTION
- Ethical statements
- This retrospective study was approved by the Institutional Review Board of Gachon University Gil Medical Center (No. GCIRB2022-187). The Institutional Review Board waived the need for informed consent.
- Study design and data collection
- We analyzed patients who were admitted to the ED for fall-related injuries using the Emergency Department-based Injury In-depth Surveillance (EDIIS) data. EDIIS is an injury investigation and monitoring project under the Korea Disease Control and Prevention Agency (KDCA). The project started in 2006, and as of 2020, 23 large hospitals in Korea are currently participating in the project. EDIIS data provide information on all injured patients who are admitted to the ED, including their demographic information, injury mechanism, and treatment outcomes. Data are collected in a standardized manner by trained investigators in each participating hospital and are then entered into the KDCA disease and health management system (https://is.kdca.go.kr/). The data undergo a quality check by third party personnel who review the appropriateness of the data.
- Inclusion and exclusion criteria
- EDIIS data from January 2019 to December 2020 were used in this study. To select fall patients, the injury mechanism (MECH) variables of the data were checked. We selected patients who satisfied the criteria of fall-related injury: patients who corresponded to C12.4 (fell, jumped, or pushed from a height <1 m), C12.5 (fell, jumped, or pushed from a height ≥1 m and <4 m), C12.6 (fell, jumped, or pushed from a height ≥4 m), or C12.7 (fell, jumped, or pushed from an unknown height). Detailed descriptions of the circumstances of injury were reviewed using the NARRATIVE variable. MECH variables that were improperly classified were also corrected based on the NARRATIVE variable. According to the Center for Disease Control and Prevention (CDC) guidelines for patients with injuries, the standard minimum height presumed to be associated with severe trauma is 20 ft (6 m), and the standard height of each floor is 10 ft (3 m). Therefore, we set the height of the third floor as ≥6 m and <9 m. Accordingly, patients who fell from a height of ≥6 m and <9 m (third floor) were included in the final analysis of this study. The injury intention (INTENT) variable was checked to exclude those whose intention could not be evaluated as well as those who had unknown intentions, were admitted to the ED due to violence or homicide, had dementia, or took drugs (such as methamphetamine). Additionally, patients with missing excessive mortality ratio-adjusted Injury Severity Score (EMR-ISS) were also excluded.
- Collected variables and definitions of terms
- The demographic information of patients (such as age and sex) was recorded. In addition, data related to the characteristics of the injury, including time of fall, season, location (indoor vs. outdoor), and the public emergency medical transport service used were analyzed. Information related to the injury outcome, such as vital signs at the ED visit, Glasgow Coma Scale scores, the severity of injury (EMR-ISS), ED outcome, admission outcome, and diagnosis (International Classification of Diseases 10th Revision [ICD-10]) were analyzed.
- Fall height was assessed as follows: if both the number of floors and fall height were recorded, the height (m) was prioritized; if only the number of floors was available, the fall height was calculated assuming a 3 m height for each floor [12]. The injury period was divided into four seasons: spring (March–May), summer (June–August), autumn (September–November), and winter (December–February). Injury time was divided into four categories: morning (06:00–11:59), afternoon (12:00–17:59), evening (18:00–23:59), and late night (00:00–05:59).
- The EMR-ISS is a scale used to assess the severity of an injury based on ICD-10 [13,14]. Excess mortality ratio is calculated as the percentage of deaths among patients diagnosed with each ICD-10 code against the expected mortality in the general population. The EMR-ISS is calculated using the summation of squares of the three highest EMR grades from all the ICD-10 codes for a particular patient: EMR-ISS = (first highest EMR grade)2 + (second highest EMR grade)2 + (third highest EMR grade)2. The severity of an injury can be classified into four groups depending on the EMR-ISS: mild (1< EMR-ISS ≤8), moderate (9≤ EMR-ISS ≤24), severe (25≤ EMR-ISS ≤74), and critical (EMR-ISS ≥75 or death). In this study, we categorized patients into the following groups based on the severity of their injury, as assessed using the EMR-ISS: mild/moderate group (<25) and severe group (≥25).
- The injury site was classified according to the ICD-10 code. In the EDIIS data, the major diagnosis for each patient was entered across 10 different variables: head (S00–S09); neck (S10–S19); chest (S20–S29); abdomen, waist, and pelvis (S30–S39); shoulder and upper arm (S40–S49); elbow and forearm (S50–S59); wrist, hand, and finger (S60–S69); hip and thigh (S70–S79); knee and lower extremity (S80–S89); and ankle and foot (S90–S99).
- Primary outcome
- Primary outcomes were to evaluate the risk factors associated with the severity of fall-related injuries from similar fall heights and assess differences in the injury site between the severe and mild/moderate groups and between the intention and non-intention groups.
- Statistical analysis
- Data were analyzed using PASW SPSS ver. 18.0 (SPSS Inc). Continuous variables are reported as medians and interquartile ranges or means and standard deviations, as appropriate. Data were compared using the Mann-Whitney U-test or Student t-test. Categorical variables are expressed as frequencies and percentages and were compared using the chi-square test or Fisher exact test. Multivariable binary logistic regression analysis was used to assess the independent predictors of the severity of the injury. All variables with a significance level of <0.10 in the univariate analysis were included in the multivariable logistic regression analysis. The backward stepwise method was used to select the final model. The Hosmer-Lemeshow test was used to assess the goodness of fit. All statistical tests were two-sided, and a P-value of <0.05 was considered significant.
METHODS
- Study population
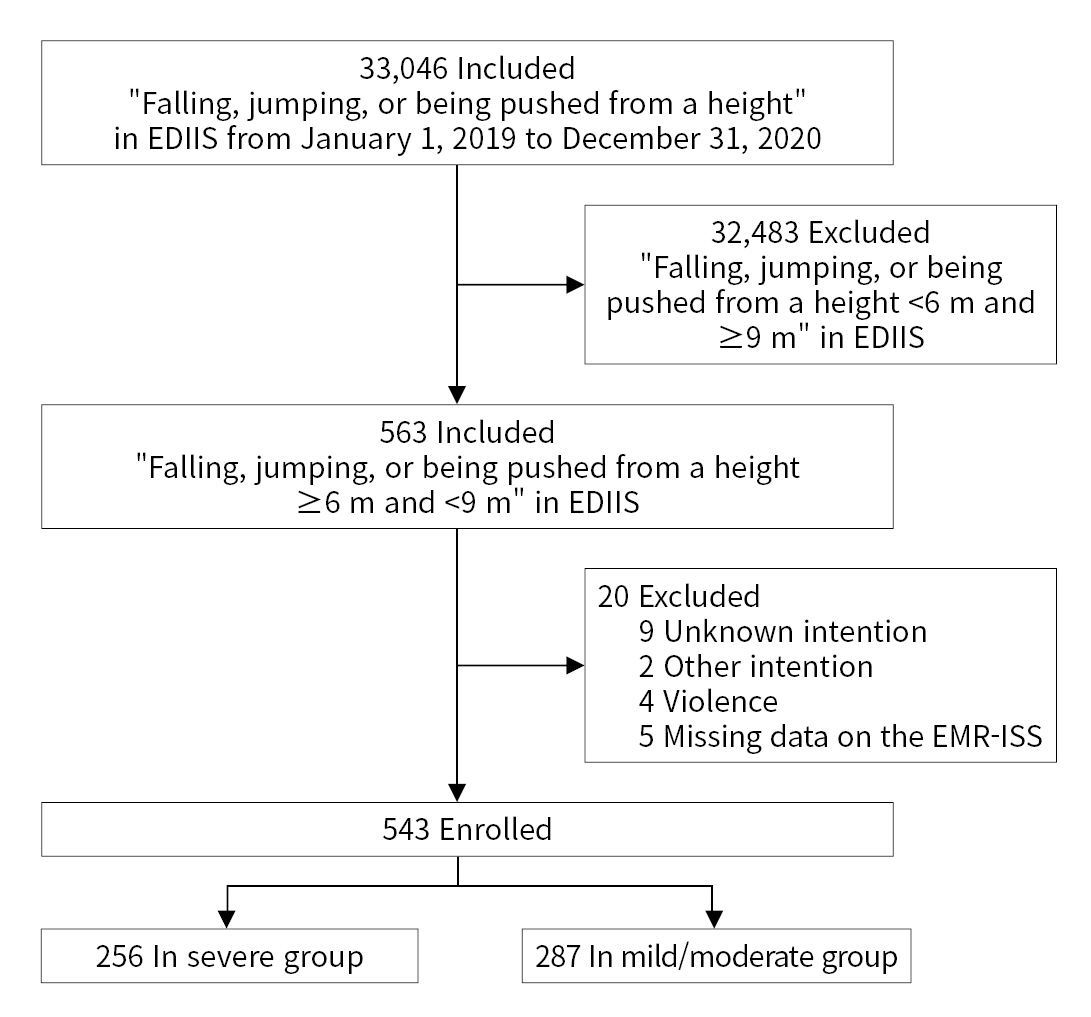
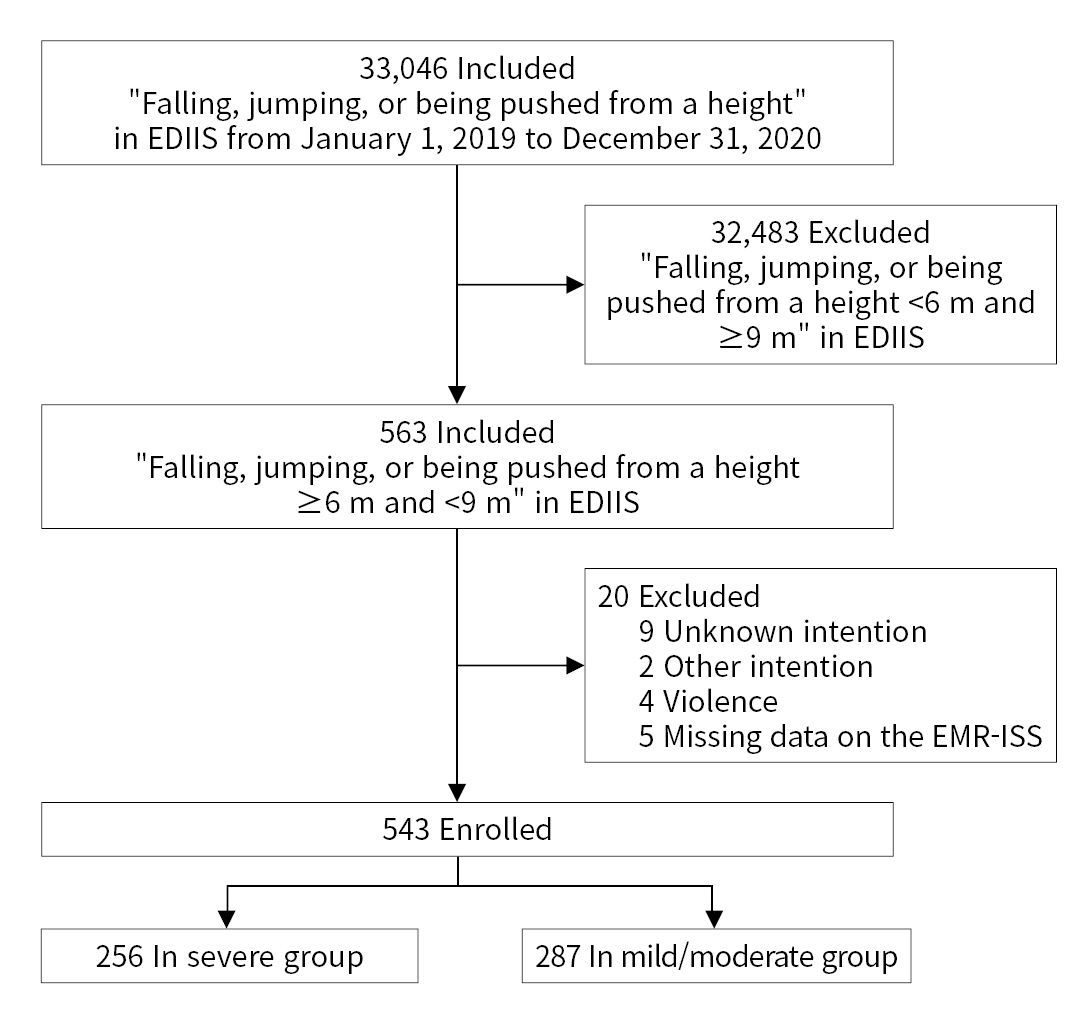
- The injury mechanism of 33,046 patients was recorded as a fall in the EDIIS database from January 1, 2019 to December 31, 2020. Of these, 563 patients who had a fall height ≥6 m and <9 m were selected initially (Fig. 1). Nine patients with unknown intention, two patients who had dementia or used methamphetamine, four patients who were victims of violence, and five patients with missing EMR-ISS were excluded, and a total of 543 patients were included in the final analysis. The severity of injury was divided according to the EMR-ISS values. A total of 256 (47%) and 287 patients (53%) were categorized in the severe and mild/moderate groups, respectively. The patients were also divided into groups according to their recorded intention. A total of 93 (17%) and 450 patients (83%) were included in the intention and non-intention groups, respectively.
- Comparison of severe and mild/moderate groups
- Table 1 lists the characteristics of the severe and mild/moderate groups. There was no difference in the percentage of male patients between the two groups (79.3% vs. 78.4%, P=0.798), and the median age of the severe and mild/moderate groups was 50 years (range, 39–60 years) and 45 years (range, 27–56 years), respectively (P<0.001). The number of patients over the age of 65 years was 45 (17.6%) in the severe group and 32 (11.1%) in the mild/moderate group (P=0.032). The mean fall height was 6.0 m (range, 6.0–7.5 m) in the severe group and 6.0 m (range, 6.0–7.0 m) in the mild/moderate group (P<0.001). The systolic blood pressure was 117.5 mmHg (range, 99.5–140 mmHg) in the severe group and 130.0 mmHg (range, 113.0–150.0 mmHg) in the mild/moderate group (P<0.001). ED death and overall deaths occurred in 16 (6.3%) and 37 patients (14.5%), respectively, in the severe group and nine (3.1%) and 16 patients (5.6%), respectively, in the mild/moderate group; the differences were statistically significant (P=0.084 and P=0.001, respectively).
- Multivariable logistic regression analysis for independent factors associated with severe injuries
- Factors related to the severity of fall injuries included fall height (odds ratio [OR], 1.638; 95% confidence interval [CI], 1.279–2.098), foot injury (OR, 0.466; 95% CI, 0.263–0.828), and systolic blood pressure <90 mmHg (OR, 2.358; 95% CI, 1.231–4.520) (Table 2). When age was divided into quartiles and the first quartile (1Q; <31.5 years) was set as the reference, the ORs of 2Q, 3Q, and 4Q were 1.747 (95% CI, 1.028–2.971), 1.545 (95% CI, 0.898–2.657), and 2.421 (95% CI, 1.405–4.171), respectively.
- Comparison of intention and non-intention groups
- Table 3 lists the characteristics of the intention and non-intention groups. The number of male patients in the intention and non-intention groups was 44 (47.3%) and 384 (85.3%), respectively (P<0.001). The median age was 33 years (range, 20–46 years) and 50 years (range, 37–60 years) in the intention and non-intention groups, respectively (P<0.001). The number of patients over the age of 65 years was six (6.5%) in the intention group and 71 (15.8%) in the non-intention group (P=0.019). A total of 28 patients (33.7%) in the intention group and 51 patients (11.6%) in the non-intention group were under the influence of alcohol when they fell (P<0.001). ED death and overall deaths occurred in seven (7.5%) and 14 patients (15.1%), respectively, in the intention group and 18 (4.0%) and 39 patients (8.7%), respectively, in the non-intention group; the differences were not statistically significant (P=0.169 and P=0.059, respectively).
- Comparison of injury site
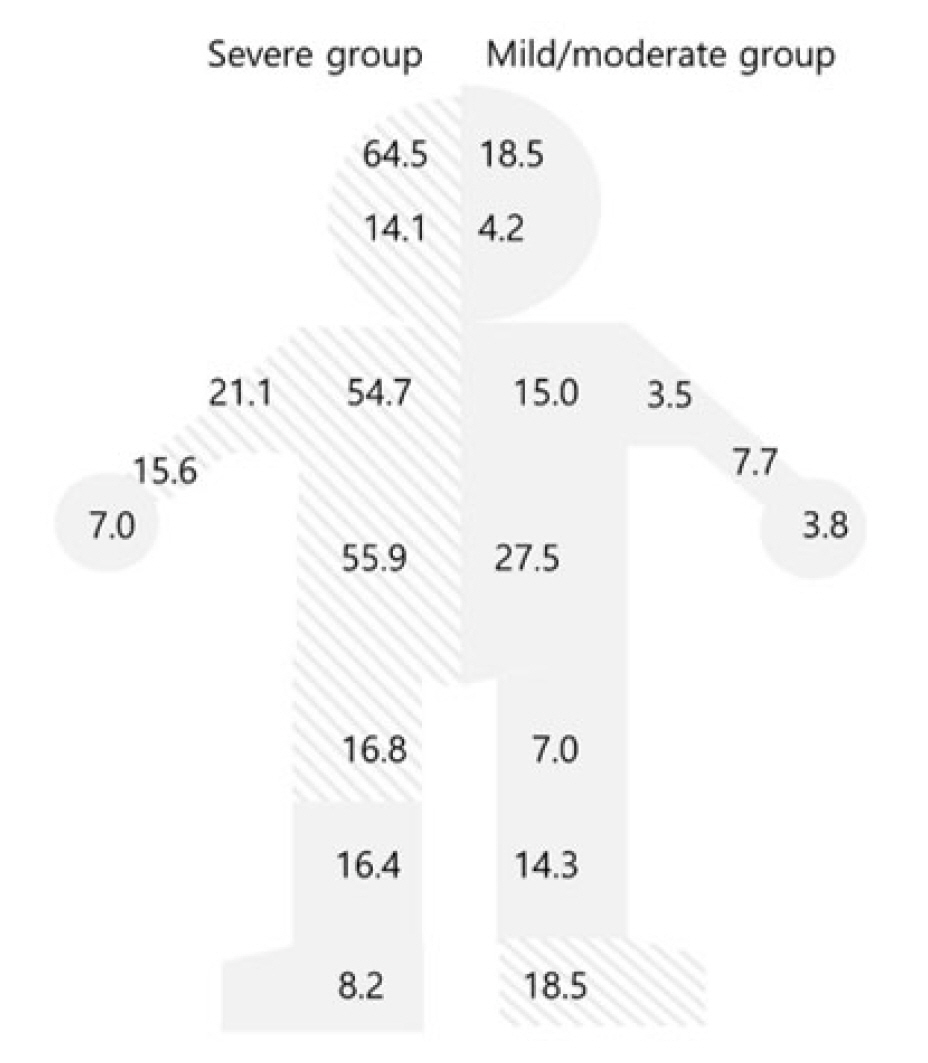
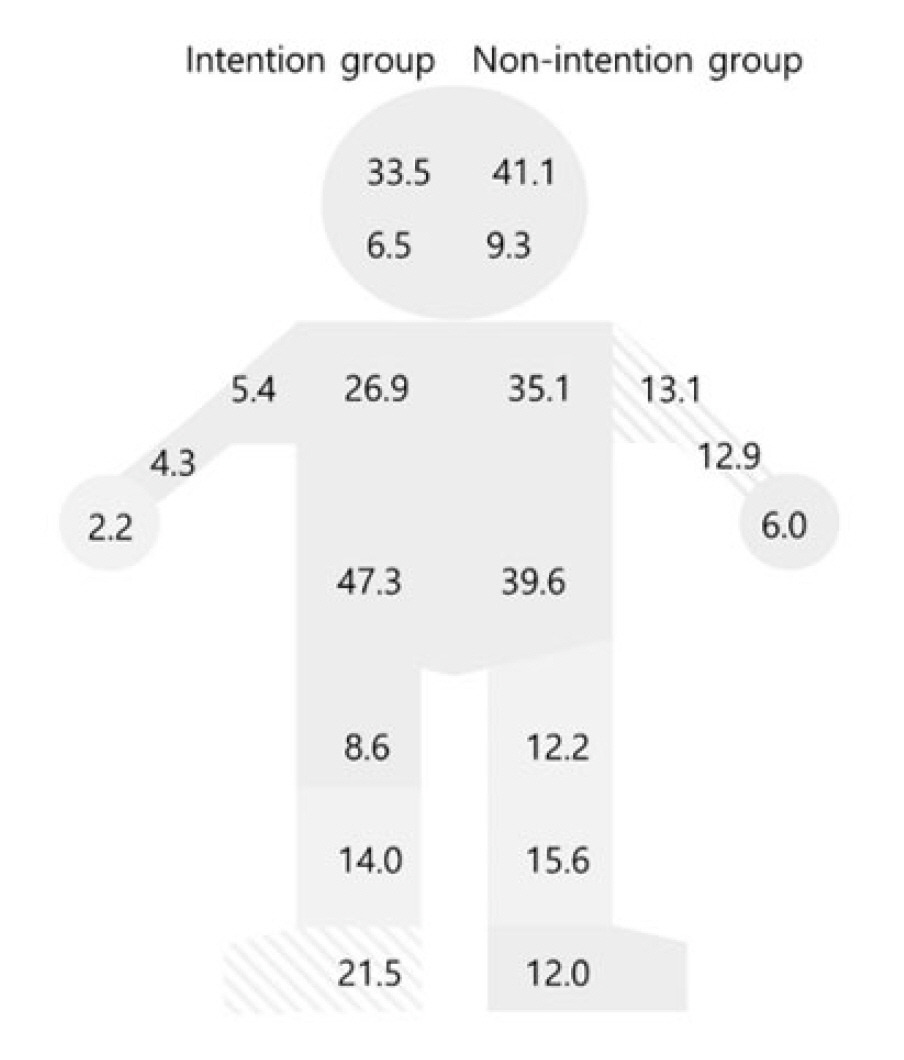
- In the severe and mild/moderate groups, the injury sites were as follows: head and neck (171 [66.8%] vs. 58 [20.2%], P<0.001), torso (183 [71.5%] vs. 104 [36.2%], P<0.001), upper extremity (96 [37.5%] vs. 34 [11.8%], P<0.001), and lower extremity (82 [32.0%] vs. 93 [32.4%], P=0.926) (Table 1). In the intention and non-intention groups, the injury sites were upper extremity (10 [10.8%] vs. 120 [26.7%], P=0.001) and lower extremity (30 [32.3%] vs. 145 [32.2%], P=0.995) (Table 3). Figs. 2 and 3 show the difference in the injury site between the severe and mild/moderate groups and the intention and non-intention groups, respectively. The incidence of forearm injuries was four (4.3%) and 58 cases (12.9%, P=0.018) and that of foot injuries was 20 (21.5%) and 54 cases (12.0%, P=0.015) in the intention and non-intention groups, respectively.
RESULTS
- In this study, we compared the general characteristics of patients who fell from a height of ≥6 m and <9 m. Although the patients fell from almost similar height, fall height was associated with injury severity. Consistent with the findings of previous studies, age was also associated with injury severity. Contrary to the findings of previous studies, intentionality was not associated with injury severity [6,7]. Here, we found that patients with foot injuries were less likely to suffer from severe injuries. Those who suffered intentional falls had a higher frequency of injuries in the lower extremity, whereas the non-intention group showed a higher frequency of injuries in the upper extremity.
- The fall height is one of the key risk factors for serious fall-related injuries [2,10]. As demonstrated in previous studies, the force of impact increases with fall height, which increases the risk of injury. In this study, we used a relatively large amount of data, which enabled comparisons between patients who fell from specific heights (≥6 m and <9 m). Although patients who fell from a similar height were compared, injury severity differed even with small differences in fall height. This suggests that fall height was the most powerful factor related to injury severity in fall-related injuries. Therefore, even if we compared patients who fell from a similar height, this study was limited because the effect of fall height could not be completely excluded. Future large-scale studies can help elucidate the effects of other risk factors by comparing patient groups with specific fall heights.
- Age is known to affect responses to stimuli, cognition, and motor skills [3]. Injury severity generally increases with the age of trauma patients [3,4]. Consistent with this, we found that age was associated with injury severity in this study. This may be because fall injuries often result from loss of balance or consciousness. When the patients were divided into four different age groups, multivariable logistic regression analysis showed that severe injuries were associated with a patient age of 31.5 to 47.0 years. A previous study showed that suicide attempts were higher in a similar age group than in other age groups [15], suggesting that a higher incidence of intentional falls might have led to more severe injuries. Previous studies have also reported that injuries were more severe in intention groups than in non-intention groups [6,7]. Contrary to these findings, we observed that intention was not associated with injury severity. This may be because in the present study, factors predicting injury severity were investigated in patients who suffered from both intentional and unintentional falls. As a result, age and intentionality may have acted as confounding factors. In previous studies where injuries were reported to be more severe in intentional falls than in unintentional falls [6,7], the mean fall height was higher in the intention group than in the non-intention group. This suggests that intentionality and fall height may have acted as confounding factors in other studies as well. Thus, further studies must be conducted to determine whether intentionality and injury severity interact with each other at similar fall heights for patients in the age group of 31.5 to 47.0 years.
- Injury sites were compared according to the injury severity. In the severe group, injuries were more frequent in the head and neck, torso, shoulder, forearm, and thigh. In contrast, the mild/moderate group showed a high frequency of foot injury. Multivariable logistic regression analysis revealed a small OR for foot injury, suggesting a low risk of severe injury in patients with foot injuries. This could mean that landing on one’s feet may help absorb the shock and reduce damage to the vital organs. Therefore, predicting injury severity in fall patients may require the evaluation of not only vital organs, but also foot injuries.
- Foot injury also has another implication for clinicians who treat unconscious fall patients. In this study, the frequency of injures in the shoulder, upper arm, and forearm was higher in the non-intention group than in the intention group. The frequency of upper extremity injuries in the non-intention group may be related to the patients’ unconscious acts to protect their body. In contrast, the frequency of foot injury was higher in the intention group than in the non-intention group. Consistent with our findings, injury sites have been shown to differ among fall patients depending on their intentionality [7]. Injuries in the lower extremity and abdomen were more common in intentional falls than in unintentional falls. Based on these findings, previous studies have suggested the "land feet first" theory [7,16]. Patients who suffer an unintentional fall have a higher risk of arm and hand injuries owing to the human body’s instinctive urge to defend themselves with their upper extremity, whereas patients who suffer an intentional fall may have a higher risk of landing on the feet, thus increasing their risk of foot injury. Thus, it would be necessary to further assess whether patients with foot injuries have intentionally fallen after alcohol or drug use.
- Limitations
- Several limitations must be considered in the interpretation of this study's findings. First, this study retrospectively analyzed prospectively collected data. Second, the fall height analyzed in this study might be distorted. We compared patients with a similar fall height to reduce the effects of fall height and evaluate other risk factors. However, the fall heights analyzed in this study were subjective height estimates provided by the patient and other personnel who reported the patient's injury status. Therefore, the values may not be accurate. Third, this study analyzed patients who fell from a height of third floors. The units to compare the fall height were meter and floor. However, as previously described, meter is a subjective numerical unit measured by witnesses. Therefore, floor was considered more objective than meter, and patients who fell from a height of third floors were analyzed. Fourth, we used diagnostic codes to identify the injury sites of patients. Therefore, the injury site variable was omitted if a diagnostic code related to the injury site was not entered after death, or if the diagnostic code entered did not specify the injury site (e.g., T148, other injury of body). Fifth, as the analyzed data were collected from large hospitals and institutions, patients with mild symptoms or those who died at the scene may not have been included. Sixth, the medical history of the patients and the material of the surface that the patients landed on after falling could not be identified or analyzed in this this. Seventh, among the various injury severity assessment tools used to assess patients in the EDIIS database, EMR-ISS had the least missing data. Thus, EMR-ISS was used in this study to analyze disease severity.
- Conclusions
- Our results showed that fall height and age were associated with severe fall-related injuries in patients with a similar fall height. Intentionality was not related to injury severity, and patients with foot injuries were less likely to suffer from serious injuries. Lower and upper extremity injuries were more common in intentional and unintentional falls, respectively.
DISCUSSION
-
Author contributions
Conceptualization: all authors; Data curation: all authors; Formal analysis: all authors; Methodology: DHK, JHW; Project administration: DHK, JHW, YBJ; Visualization: DHK, JHW; Writing–original draft: DHK, JHW, YBJ; Writing–review & editing: JSC, JHJ, JYC, WSC. All authors read and approved the final manuscript
-
Conflicts of interest
The authors have no conflicts of interest to declare.
-
Funding
This study was supported by a fund from the Research of Korea Disease Control and Prevention Agency (KDCA) (No. 2831-304-320-01).
-
Data availability
The 2019 data of this study are openly available on the KDCA website at https://www.kdca.go.kr/injury/biz/injury/recsroom/rawDta/rawDtaDwldMain.do. Restrictions apply to the availability of the 2020 data. The 2020 data of this study are available from KDCA with their permission.
ARTICLE INFORMATION
Odds ratios are calculated using a backward stepwise logistic regression analysis. The covariates included in this analysis are sex, age group, mental status, occurrence of abnormal heart rate, intentional fall, foot injuries, occurrence of low body temperature, SBP <90 mmHg, and fall height.
CI, confidence interval; SBP, systolic blood pressure.
- 1. Korea Disease Control and Prevention Agency (KDCA). Emergency Department-based Injury In-depth Surveillance. KDCA; 2020.
- 2. Seo KS, Park ST, Ha WS, et al. The prognostic significance of Injury Severity Score and height of fall in free fall patients. J Korean Soc Traumatol 2009;22:12–17.
- 3. James MK, Victor MC, Saghir SM, Gentile PA. Characterization of fall patients: does age matter? J Safety Res 2018;64:83–92. ArticlePubMed
- 4. Demetriades D, Murray J, Brown C, et al. High-level falls: type and severity of injuries and survival outcome according to age. J Trauma 2005;58:342–5. ArticlePubMed
- 5. Ren J, Waclawczyk A, Hartfield D, et al. Analysis of fall injuries by body mass index. South Med J 2014;107:294–300. ArticlePubMed
- 6. Piazzalunga D, Ruberta F, Fugazzola P, et al. Suicidal fall from heights trauma: difficult management and poor results. Eur J Trauma Emerg Surg 2020;46:383–8. ArticlePubMedPDF
- 7. Kang BH, Jung K, Huh Y. Suicidal intent as a risk factor for mortality in high-level falls: a comparative study of suicidal and accidental falls. Clin Exp Emerg Med 2021;8:16–20. ArticlePubMedPMCPDF
- 8. Petaros A, Slaus M, Coklo M, Sosa I, Cengija M, Bosnar A. Retrospective analysis of free-fall fractures with regard to height and cause of fall. Forensic Sci Int 2013;226:290–5. ArticlePubMed
- 9. Casali MB, Battistini A, Blandino A, Cattaneo C. The injury pattern in fatal suicidal falls from a height: an examination of 307 cases. Forensic Sci Int 2014;244:57–62. ArticlePubMed
- 10. Alizo G, Sciarretta JD, Gibson S, et al. Fall from heights: does height really matter? Eur J Trauma Emerg Surg 2018;44:411–6. ArticlePubMedPDF
- 11. Icer M, Guloglu C, Orak M, Ustundag M. Factors affecting mortality caused by falls from height. Ulus Travma Acil Cerrahi Derg 2013;19:529–35. ArticlePubMed
- 12. Centers for Disease Control and Prevention. Guidelines for field triage of injured patients: recommendations of the National Expert Panel on Field Triage, 2011. MMWR 2012;61(RR-1):1–20.
- 13. Kim J, Shin SD, Im TH, et al. Development and validation of the excess mortality ratio-adjusted Injury Severity Score using the International Classification of Diseases 10th edition. Acad Emerg Med 2009;16:454–64. ArticlePubMed
- 14. Choi SW, Woo JH, Hyun SY, Jang JH, Choi WS. Factors associated with injury severity among users of powered mobility devices. Clin Exp Emerg Med 2021;8:103–10. ArticlePubMedPMCPDF
- 15. Yi K, Na RJ, Ahn MH, Lim A, Hong JP. Trends in prevalence of suicidal idea, attempt and suicide rate in Korea, 2006-2011. Anxiety Mood 2012;8:141–5.
- 16. Teh J, Firth M, Sharma A, Wilson A, Reznek R, Chan O. Jumpers and fallers: a comparison of the distribution of skeletal injury. Clin Radiol 2003;58:482–6. ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite