Articles
- Page Path
- HOME > J Trauma Inj > Volume 31(3); 2018 > Article
-
Case Report
Iatrogenic Delayed Aortic Injury Following a Surgical Stabilization of Flail Chest - Junepill Seok, M.D., Hyun Min Cho, M.D., Seon Hee Kim, M.D., Ho Hyun Kim, M.D.
-
Journal of Trauma and Injury 2018;31(3):174-176.
DOI: https://doi.org/10.20408/jti.2018.037
Published online: December 31, 2018
- 2,758 Views
- 41 Download
- 1 Crossref
Department of Trauma and Surgical Critical Care, Pusan National University Hospital, Busan, Korea
- Correspondence to: Hyun Min Cho, M.D., Department of Trauma and Surgical Critical Care, Pusan National University Hospital, 179 Gudeok-ro, Seo-gu, Busan 49241, Korea, Tel: +82-51-240-7369, Fax: +82-51-240-7719, E-mail: csking1@daum.net
• Received: August 28, 2018 • Revised: November 8, 2018 • Accepted: November 13, 2018
Copyright © 2018 The Korean Society of Trauma
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- Most of aortic injuries after blunt chest trauma usually occur at the aortic isthmus and are identified in the emergency department soon after arrival. Delayed aortic injures by fractured posterior ribs, however, are relatively rare and have been reported only a few times. We recently experienced an iatrogenic descending aortic injury sustained as a result of a direct puncture by a sharp rib end after surgical stabilization of rib fractures.
- Traumatic injury of the aorta is a life-threatening condition in which survival depends on early diagnosis and treatment. It usually occurs at the aortic isthmus just distal to the left subclavian artery by rapid deceleration [1,2], but other sites can be affected. Direct damage to the aorta by fractured ribs on scene which requires emergent operation is identified in the emergency department soon after arrival to the hospital [3,4]. Delayed aortic injuries after blunt trauma, however, have been reported only a few times [5–11]. We describe the case of an iatrogenic aortic injury sustained as a result of a direct puncture by a sharp rib end after surgical stabilization of rib fractures (SSRF).
INTRODUCTION
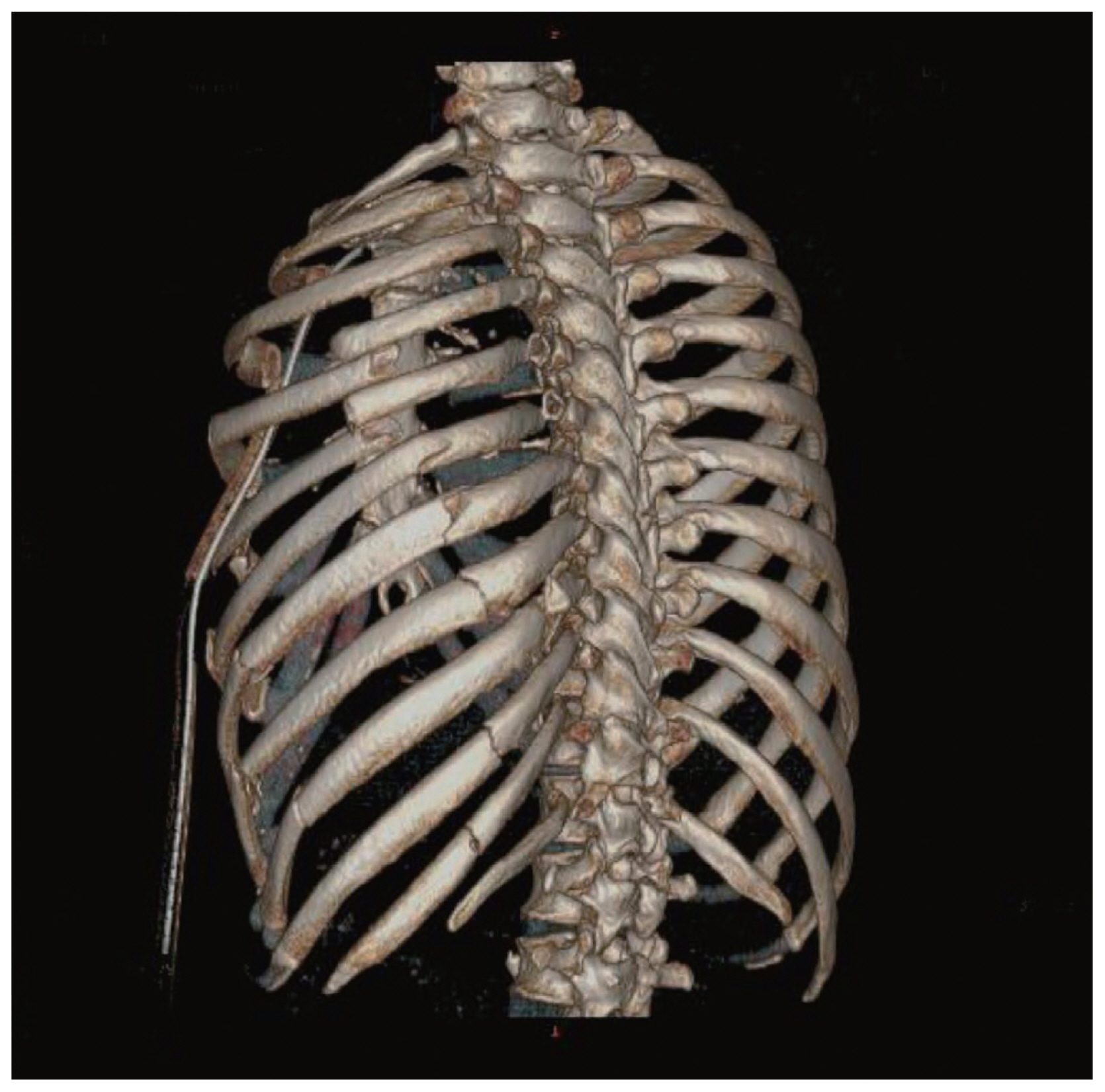
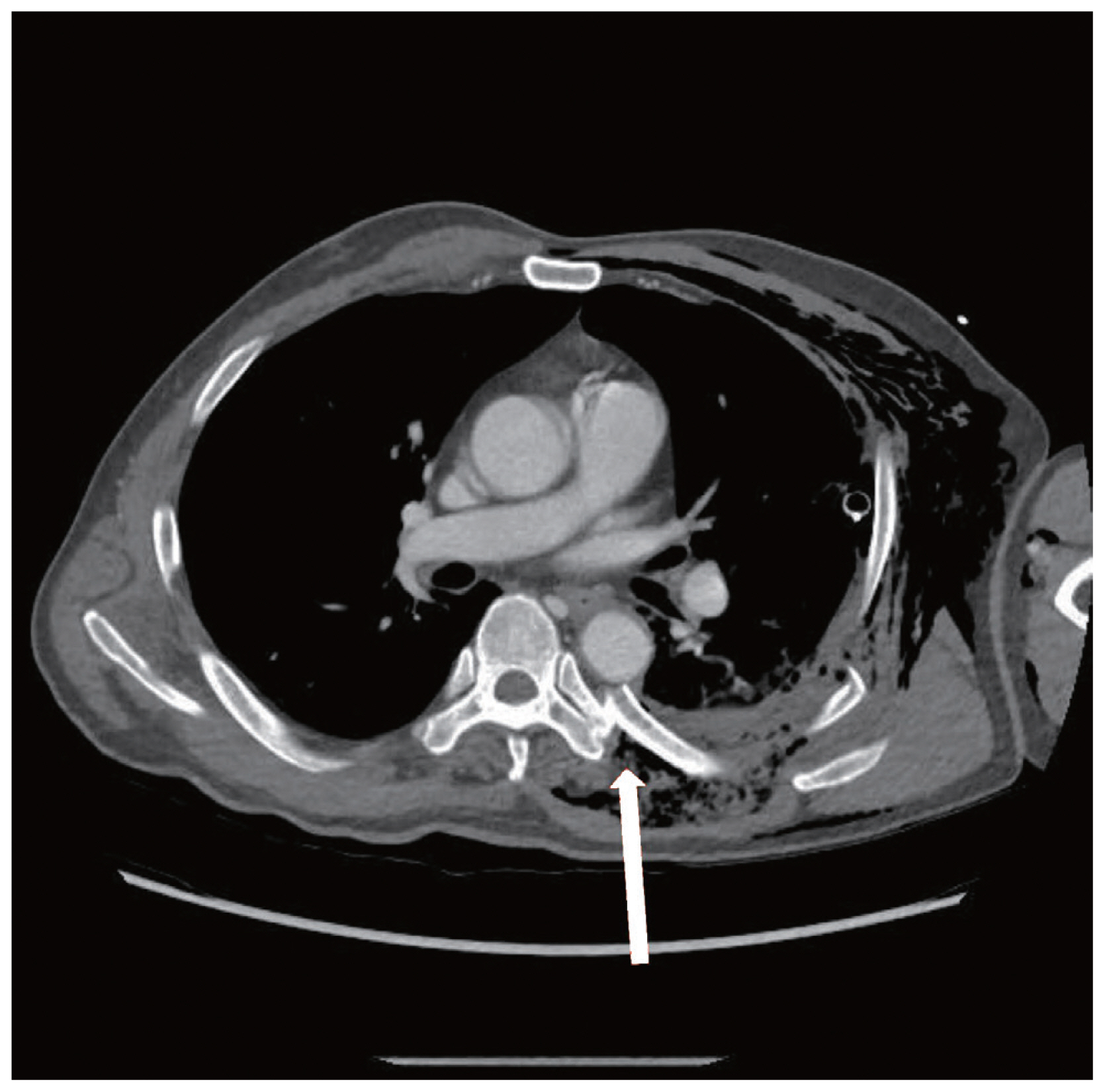
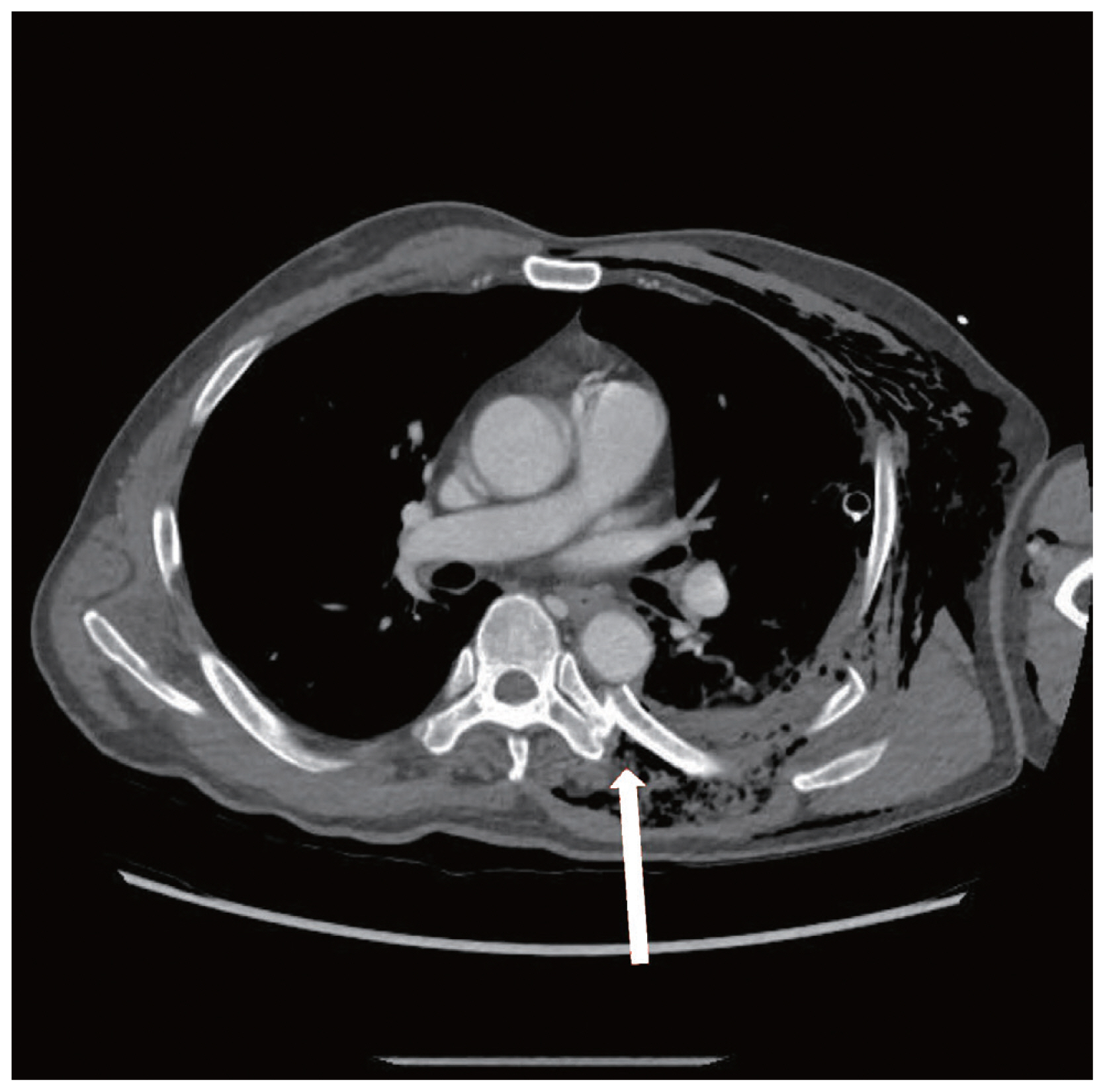
- A 61 years old male admitted to the emergency department with respiratory failure and left arm amputation after an accident. Chest computed tomography (CT) revealed multiple rib fractures with traumatic hemopneumothorax on the left thorax. Segmental fractures of the 4th to 9th ribs were identified, especially posterior ends of the 5th and 6th rib fractures were dislocated into the thoracic cavity, adjacent to the descending thoracic aorta (Figs. 1, 2). The patient was intubated because of respiratory failure by flail chest, and a drainage thoracic catheter was placed. Only 200 mL of blood was drained initially through the drainage thoracic catheter. The patient underwent emergent operation for the left arm anastomosis.
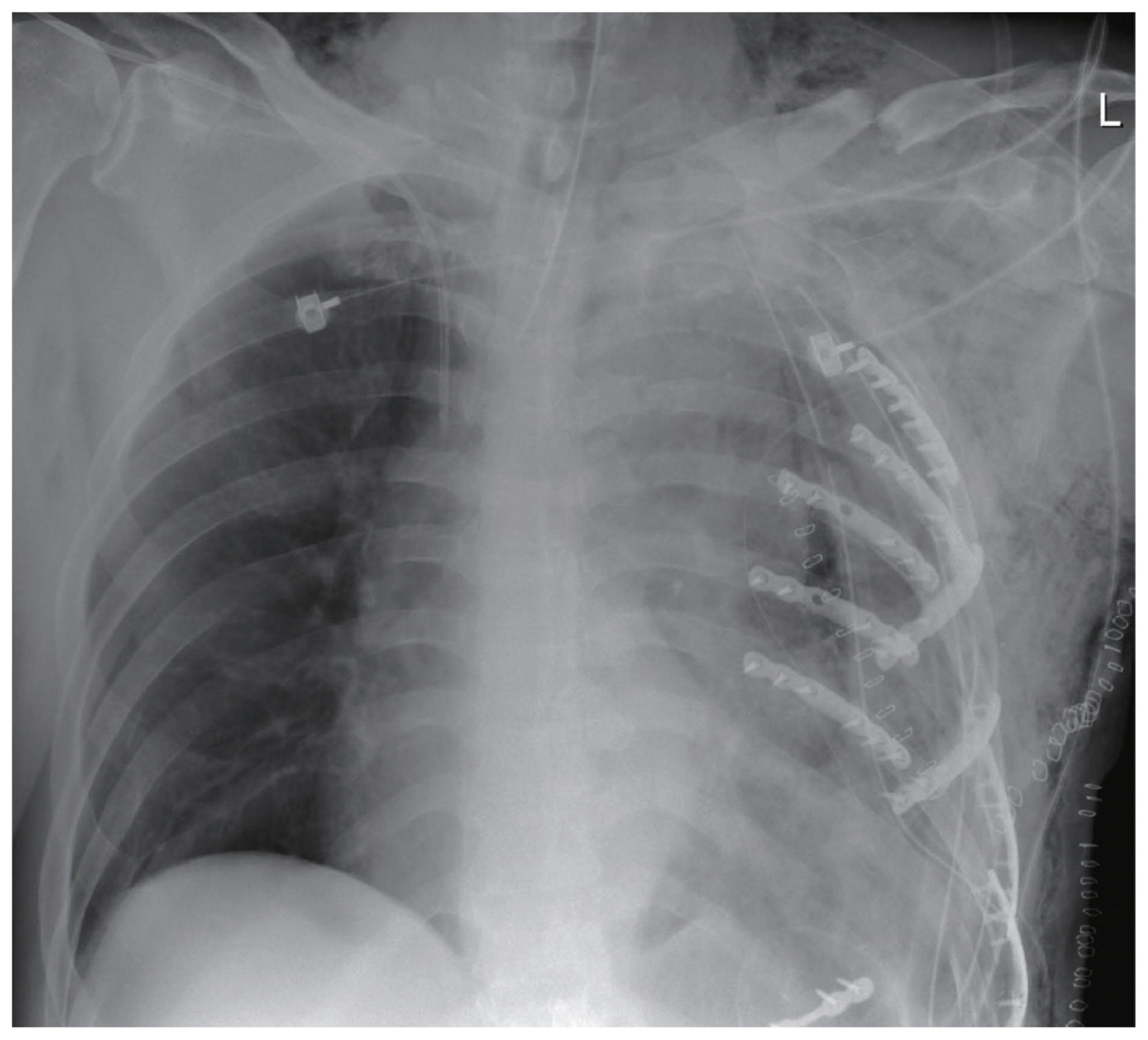
- On the hospital day 3, the patient underwent SSRF for the flail chest. On the operation field, lateral ends of the 4th to 8th rib fractures were fixed with plates and screws. Posterior ends of rib fractures were not stabilized because they were too closely located to the thoracic vertebrae (Fig. 2). After the operation, the patient was hemodynamically stable and transferred to the surgical intensive care unit. Soon after, the patient became hypotensive and suddenly fell into deep shock after taking a postoperative chest X-ray (Fig. 3). More than 2,000 mL of massive blood poured out through the drainage thoracic catheter. We promptly reopened the operation wound on the bed. After evacuating large amount of hematoma, we found that the posterior end of the 6th rib fracture penetrated the descending aorta. Finger tamponade was performed, and then injured aortic wall was repaired with a pledgeted suture of 4-0 prolene in a U fashion. After emergent bedside procedure, the patient was transferred to the operating room again. The posterior ends of the 5th and 6th rib fractures were rongeured off and smoothened. The patient was discharged 4 months later.
CASE REPORT
- Delayed aortic injuries due to fractured ribs have been reported infrequently. Park et al. [7] suggested two possible mechanisms which are able to worsen this situation, temporary clot formation of the penetrated aortic wall and physical movements of the patient after initial trauma. Marco and Gregory [9] reported a case of the delayed aortic injury on the 3rd hospital day, they suggested that the injured aortic wall initially formed a pseudoaneurysm at scene without active bleeding. Kigawa et al. [5] also reported a delayed aortic injury after changing the body position of a patient with flail chest on the 10th hospital day. In our case, the patient initially did not show the clinical manifestations of aortic injury. Although several posterior ends of rib fractures were dislocated toward the descending thoracic aorta (Fig. 2), only subclinical amount of hemorrhage was identified through the drainage thoracic catheter, and the patient became hemodynamically stable after being intubated. Right after the SSRF for the flail chest on the 3rd hospital day, however, the descending thoracic aorta was penetrated by posterior ends of rib fractures. We only stabilized lateral ends of rib fractures at that time, and this procedure moved the posterior end of the 6th rib fracture closer to the descending aorta, and finally the aorta was penetrated.
- Based on the result, this patient already had been exposed to high risk of delayed aortic injury by rib fractures regardless of the SSRF, although the SSRF definitely caused disastrous consequences. When we decided to stabilize rib fractures, we should have considered how to manage posterior ends of rib fractures during the operation. This case suggests that if posterior rib fractures are severely dislocated into the thoracic cavity and closely located to the descending thoracic aorta on the initial chest CT, care should be taken to prevent adverse outcome.
DISCUSSION

- 1. Smith RS, Chang FC. Traumatic rupture of the aorta: still a lethal injury. Am J Surg 1986;152:660–3.ArticlePubMed
- 2. Schulman CI, Carvajal D, Lopez PP, Soffer D, Habib F, Augenstein J. Incidence and crash mechanisms of aortic injury during the past decade. J Trauma 2007;62:664–7.ArticlePubMed
- 3. Plume S, DeWeese JA. Traumatic rupture of the thoracic aorta. Arch Surg 1979;114:240–3.ArticlePubMed
- 4. Carter RR, Orr NT, Minion DJ, Xenos ES. Aortic injury from posterior rib fracture. Eur J Cardiothorac Surg 2011;39:138, ArticlePubMedPDF
- 5. Kigawa I, Fukuda I, Fujii Y, Yamabuki K. A sharp edge of the fractured ribs caused the aortic injury at body-position change: a case report. Nihon Kyobu Geka Gakkai Zasshi 1992;40:1116–20.PubMed
- 6. Bruno VD, Batchelor TJ. Late aortic injury: a rare complication of a posterior rib fracture. Ann Thorac Surg 2009;87:301–3.ArticlePubMed
- 7. Park HS, Ryu SM, Cho SJ, Park SM, Lim SH. A treatment case of delayed aortic injury: the patient with posterior rib fracture. Korean J Thorac Cardiovasc Surg 2014;47:406–8.ArticlePubMedPMCPDF
- 8. Tsai FC, Chang YS, Lin PJ, Chang CH. Blunt trauma with flail chest and penetrating aortic injury. Eur J Cardiothorac Surg 1999;16:374–7.ArticlePubMedPDF
- 9. Marco JV, Gregory JS. Posterior fracture of the left sixth rib causing late aortic laceration: case report. J Trauma 1997;42:736–7.ArticlePubMed
- 10. Kano M, Chikugo F, Fujimoto E. Delayed aortic injury caused by sharp rib fracture. Asian Cardiovasc Thorac Ann 2014;22:500, ArticlePubMed
- 11. Boyles AD, Taylor BC, Ferrel JR. Posterior rib fractures as a cause of delayed aortic injury: a case series and literature review. Injury Extra 2013;44:43–5.Article
REFERENCES
Figure & Data
References
Citations
Citations to this article as recorded by 
- Surgical Stabilisation of Traumatic Rib Fractures with Chronic, Residual Type A Aortic Dissection
Kieran J. Matic, Rajkumar Cheluvappa, Selwyn Selvendran
Healthcare.2021; 9(4): 392. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite