An Early Experience of Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) in the Republic of Korea: A Retrospective Multicenter Study
Article information
Abstract
Purpose
This retrospective multicenter study analyzed trauma patients who underwent resuscitative endovascular balloon occlusion of the aorta (REBOA) in the Republic of Korea.
Methods
This study was conducted from February 2017 to May 2018 at three regional trauma centers in the Republic of Korea. The patients were divided into two groups (cardiopulmonary resuscitation [CPR] and No-CPR) for comparative analysis based on two criteria (complication and mortality) for logistic regression analysis (LRA).
Results
There were significant differences between the CPR and No-CPR groups in mortality (p=0.003) and treatment administered (p=0.016). By LRA for complications, total occlusion has significantly lesser risk than intermittent or partial occlusion in both univariate (odds ratio [OR] 0.06, 95% confidence interval [CI] 0.00-0.36, p=0.01) and multivariate (OR 0.05, 95% CI 0.00-0.38, p=0.01) analyses. The Rescue had a higher risk than the Coda or Reliant in univariate analysis (OR 4.91, 95% CI 1.14-34.25, p=0.05); however, it was not statistically significant in multivariate analysis (OR 6.98, 95% CI 1.03-74.52, p=0.07). By LRA for mortality, the CPR group was the only variable that had a significantly higher risk of mortality than the No-CPR group in both univariate (OR 17.59, 95% CI 3.05-335.25, p=0.01), and multivariate (OR 24.92, 95% CI 3.77-520.51, p=0.01) analyses.
Conclusions
This study was conducted in the early stages of REBOA implementation in the Republic of Korea and showed conflicting results from studies conducted by multiple institutions. Therefore, additional research with more accumulated data is needed.
INTRODUCTION
In trauma patients, hemorrhage is one of the most fatal conditions, and it is the second leading cause of traumatic mortality [1]. A total of 30-40% of traumatic patients have died from hemorrhage [2]. Worldwide, 1,481,700 people die from traumatic hemorrhage yearly, and the years of life lost from traumatic hemorrhage are 74,568,000 years [3].
Resuscitative endovascular balloon occlusion of the aorta (REBOA) has been developed to control hemodynamically unstable hemorrhagic shock patients and to maintain brain and coronary perfusion [4,5]. Emergency resuscitative thoracotomy (ERT), which was previously performed, can be indicated for a single penetrating injury; however, for blunt injuries, there are many debates on performing ERT [6]. Some authors argue that REBOA can replace ERT in select cases [4,7]. In places, such as the Republic of Korea, where most traumatic patients experience blunt traumas (90.8%), REBOA is becoming important for hemorrhagic shock patients [8]. However, REBOA has several disadvantages [9]: 1) It is extremely time-dependent. 2) It has limited indications in patients with abdominal or pelvic hemorrhage who have a detectable pulse but whose systolic blood pressure remains 80 mmHg or less despite resuscitative efforts [10]. 3) It has many complications, such as distal ischemia and mortality. Nevertheless, because REBOA can play an important role in saving the time required to proceed to the next stage of treatment in blunt trauma patients, discussions to find an appropriate indication for REBOA and reduce its complications are under way.
As a result, in this multicenter retrospective study, we analyzed trauma patients who underwent REBOA according to their mortality, development of complications, and cardiopulmonary resuscitation (CPR). Furthermore, we tried to identify other variables that can affect the risk of complications and mortality. We hypothesized that the type of REBOA and type of catheter used may affect the risk for complications and mortality.
Group for Resuscitative Endovascular and Advanced treatment on Trauma (GREAT)
GREAT is an academic society in the Republic of Korea that studies endovascular treatment of trauma, including REBOA, and conducts research and education. The first meetings began in December 2016, and the data collection for this study was conducted by GREAT. GREAT has developed an education program for REBOA called ET-REBOA. ET-REBOA was first started in May 2018 and is currently being implemented as a Korean Association for Research, Procedures, and Education on Trauma (KARPET) education program (http://karpet.or.kr).
METHODS
Population
This was a retrospective multicenter study conducted from February 2017 to May 2018 at three regional trauma centers belonging to tertiary medical institutions in the Republic of Korea. We collected data of patients who underwent REBOA using the registry of Yonsei University Wonju Severance Christian Hospital, Dankook University Hospital, and Gachon University Gil Medical Center. The patients were divided into two groups (CPR and No-CPR) for comparative analysis and were divided based on two criteria (survival and mortality, occurrence and nonoccurrence of complication) for logistic regression analysis (LRA). The CPR group comprised patients who received CPR, while the No-CPR group included those who did not receive CPR. The demographic data, injury severity score (ISS), injury type, reason for REBOA, access method (cut down, palpitation, ultrasonography), access site, confirmation of the balloon position, type of catheter, type of REBOA, zone of REBOA, time of occlusion, treatment after REBOA, name of the provider, and information on development of complications and mortality was obtained from the electronic medical records of the study patients. The mechanisms of injury were classified as blunt or penetrating. The reasons for REBOA were classified as low extremity or pelvis injury, abdomen or chest injury, and multiple injuries. The treatment after REBOA was classified as surgery, angioembolization, both surgery and angioembolization, and no treatment.
REBOA
All patients received REBOA in the hospital. In most cases, REBOA was performed based on the judgment of the trauma surgeon on duty, but in two cases, it was performed by an emergency physician or vascular surgeon. We used a Coda® balloon 14 Fr catheter (Cook Medical, Bloomington, USA), Reliant® balloon 12 Fr catheter (Medtronic, Minneapolis, USA), and Rescue balloon® 7 Fr catheter (Tokai Medical Products, Aichi, Japan). In all cases, the access site was the femoral artery, and we used both the left and right femoral arteries. The REBOA zone was confirmed via radiography, C-arm, and ultrasonography, but two cases were not confirmed (blind). Total and partial or intermittent occlusion was performed depending on the patient’s condition. The duration of REBOA was measured from the first balloon inflation to the final deflation.
Statistical analysis
All statistical analyses were performed using R Statistical Software (version 3.6.3; R Foundation for Statistical Computing, Vienna, Austria). For the comparison of trauma patients who underwent REBOA with or without CPR, the Student’s t-test was used for continuous variables, based on the normal distribution, which was confirmed using the Shapiro-Wilk test, and the Fisher exact test was used to compare categorical variables. Two LRA models were created with mortality and complications as dependent variables. All LRA were performed as univariate and multivariate analyses. The independent variables of these models were age, sex, ISS, type of REBOA, type of catheter, and CPR. All results of LRA were expressed as odds ratios (ORs) and 95% confidence intervals (CIs). For all statistical analyses, p<0.05 was considered statistically significant.
RESULTS
Patient selection and characteristics
The flowchart of this study is summarized in Fig 1. During the study period, 56 patients received REBOA. Two patients were excluded due to failure; consequently, 54 patients were eligible for this study. Twenty-four patients received CPR. Among them, only one patient survived (4.2%). In the No-CPR group, 18 patients survived (60.0%). A total of 19 patients survived (35.2%), and 35 patients died (64.8%). Mortality was significantly higher in the CPR group (p=0.003).
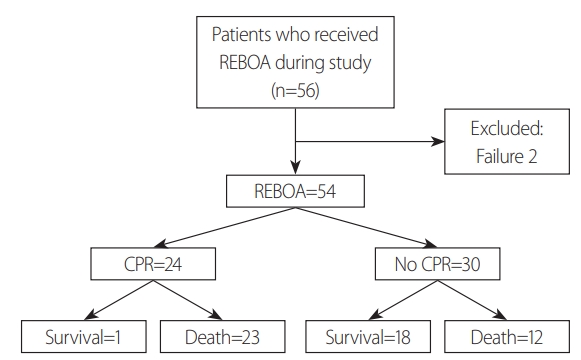
Flowchart of this study. REBOA: resuscitative endovascular balloon occlusion of the aorta, CPR: cardiopulmonary resuscitation
Other characteristics of patients according to the CPR status are summarized in Table 1. There were no significant differences in sex (p=0.729), age (p=0.299), ISS (p=0.755), injury type (p=1.000), multiple injury (p=1.000), low extremity injury (p=0.842), pelvic bone fracture (p=0.520), intra-abdominal injury (p=1.000), intra-chest injury (p=0.842), access method (p=0.652), access site (p=0.927), confirmation of balloon position (p=0.337), type of catheter (p=0.740), type of REBOA (p=0.207), zone (p=0.877), time of occlusion (p=0.494), provider (p=0.359), and occurrence of complications (p=0.282) between the CPR and No-CPR groups. Only one patient received REBOA due to penetrating injury. REBOA balloons were confirmed by radiography in most cases (90.7%), and there were two cases in which REBOA balloons were placed in Zone 2. On the other hand, there were significant differences in mortality (p=0.003) and following treatment (p=0.016) between the CPR group and the No-CPR group.
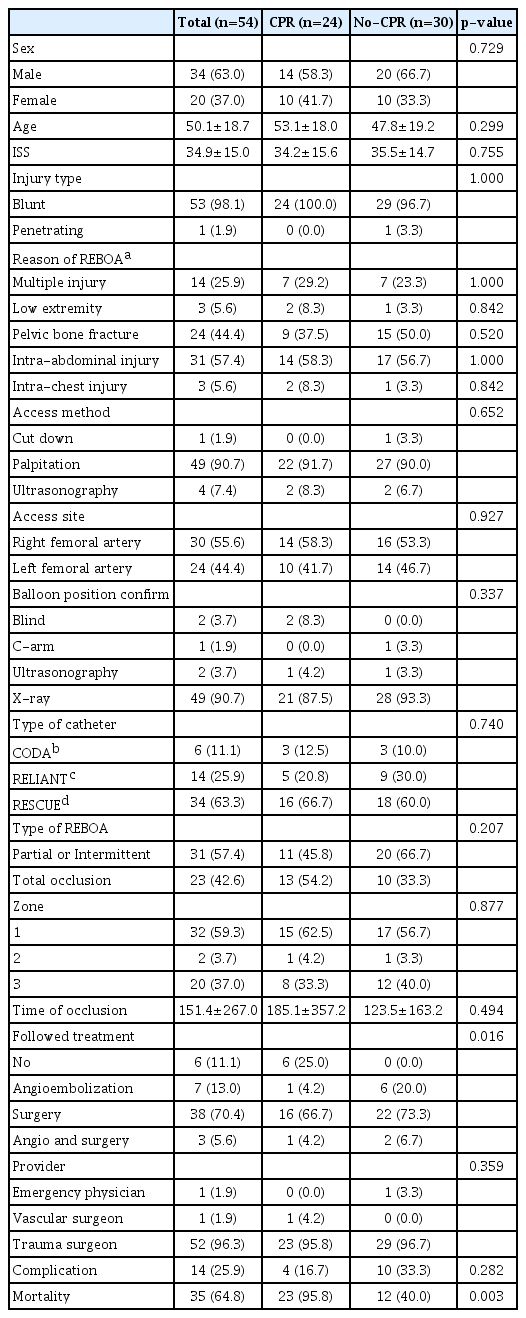
Patient characteristics according to CPR status
Logistic regression analysis for complications
Univariate and multivariate LRA for the occurrence of complications were performed. Age was not statistically significant in both univariate (OR 1.00, 95% CI 0.97-1.04, p=0.83) and multivariate (OR 1.00, 95% CI 0.96-1.05, p=0.92) analyses. Males had a significantly higher risk of complications than females in both univariate (OR 4.91, 95% CI 1.14-34.25, p=0.05) and multivariate (OR 11.3, 95% CI 2.01-100.64, p=0.01) analyses, and the effect was reinforced in multivariate analysis. ISS was not statistically significant in both univariate (OR 0.99, 95% CI 0.95-1.03, p=0.63) and multivariate (OR 0.99, 95% CI 0.93-1.05, p=0.85) analyses. Total occlusion had a significantly lesser risk than intermittent or partial occlusion in both univariate (OR 0.06, 95% CI 0.00-0.36, p=0.01) and multivariate (OR 0.05, 95% CI 0.00-0.38, p=0.01) analyses, and the effects were similar between univariate and multivariate analyses. The Rescue had a higher risk than Coda or Reliant in univariate analysis (OR 4.91, 95% CI 1.14-34.25, p=0.05), but it was not statistically significant in multivariate analysis (OR 6.98, 95% CI 1.03-74.52, p=0.07). However, it cannot be easily ignored because 95% CI of multivariate analysis does not include 1. Finally, the No-CPR group was not statistically significant compared to the CPR group in both univariate (OR 2.50, 95% CI 0.71-10.35, p=0.17), and multivariate (OR 2.43, 95% CI 0.42-16.37, p=0.33) analyses. The p-value of Hosmer and Lemeshow goodness of fit test for this model was 0.901, and the area under the receiver operating characteristic curve (AUC) was 0.893, which means that this LRA model explains the data of this study well.
Logistic regression analysis for mortality
Univariate and multivariate LRA for mortality were also performed. Age was not statistically significant in both univariate (OR 1.00, 95% CI 0.96-1.03, p=0.79) and multivariate (OR 1.00, 95% CI 0.96-1.05, p=0.92) analyses. Male sex was not statistically significant compared to female sex in both univariate (OR 1.08, 95% CI 0.31-4.07, p=0.91) and multivariate (OR 1.01, 95% CI 0.22-4.91, p=0.99) analyses. ISS was not statistically significant in both univariate (OR 0.99, 95% CI 0.94-1.03, p=0.53) and multivariate (OR 0.98, 95% CI 0.92-1.03, p=0.40) analyses. Total occlusion was not statistically significant compared to intermittent or partial occlusion in both univariate (OR 1.01, 95% CI 0.29-3.47, p=0.98) and multivariate (OR 2.26, 95% CI 0.48-12.04, p=0.31) analyses. Rescue was not statistically significant compared to Coda or Reliant in both univariate (OR 1.08, 95% CI 0.31-4.07, p=0.91) and multivariate (OR 1.26, 95% CI 0.28-5.98, p=0.76) analyses. The CPR group was the only variable that had a significantly higher risk for mortality than the No-CPR group in both univariate (OR 17.59, 95% CI 3.05-335.25, p=0.01) and multivariate (OR 24.92, 95% CI 3.77-520.51, p=0.01) analyses. The p-value of Hosmer and Lemeshow goodness of fit test for this model was 0.762, and AUC was 0.809. Therefore, the LRA model for mortality fits the data of this study.
DISCUSSION
When we compared the CPR and No-CPR groups in trauma patients who underwent REBOA within our study, no variables, except mortality and following treatment, showed significant differences between the two groups. Chen et al. [11] reported that only 2.2% of traumatic cardiac arrest patients survived for at least 30 days, and ISS above 16 and total resuscitation length above 20 minutes were unfavorable factors for mortality. In our study, the mean ISS was 34.9±15.0. Consequently, CPR is an independent factor influencing mortality. In the CPR group, six patients could not receive the following treatment because the patients had expired. More patients in the No-CPR group received other treatments, such as surgery, angiographic embolization, or both than those in the CPR group.
The main reason for REBOA is intra-abdominal injury (57.4%). However, if we check each injury type, pelvic bone fracture (44.4%) was the most common reason for REBOA, and liver injury was the second most common reason. The injury type distribution by the detailed organ is described in Table 2. Fourteen patients (25.9%) had multiple organ injuries, and there was no significant difference between the CPR and the No-CPR groups (p=1.000). The majority of our cases showed intra-abdominal organ injury or pelvic bone fracture. In 3 cases we performed REBOA on patients with lung injury. Two of them had multiple organ (spleen, liver, and lung) injuries, and the other had solitary lung injury. REBOA is indicated mostly in patients with life-threatening hemorrhagic injuries below the diaphragm [12], and the performance of REBOA in thoracic trauma patients with or without other torso injuries has been debated [13]. Ordoñez et al. [14] suggested that the combination of REBOA and ERT could be useful in patients with non-compressible torso hemorrhage secondary to penetrating chest trauma in their 7-case series report. However, in our study, all patients with lung injury were injured from blunt trauma; therefore, it is better to be careful about implementation of REBOA in patients with thoracic injuries.

The injured organ of the patients
Fourteen patients developed complications, as described in Table 3. Postoperative bleeding was the highest in four cases, followed by lower limb ischemia in two cases. There was one case each for bowel ischemia, sigmoid colon perforation, acute respiratory distress syndrome, lung atelectasis, pleural effusion, pulmonary thromboembolism, stress-induced cardiomyopathy, and pseudoaneurysm. There are many complications associated with REBOA. The reported complications of REBOA included femoral arterial complications (disruption, dissection, pseudoaneurysm, hematoma, thromboembolism), extremity ischemia, aortoiliac complication (intimal tear, dissection, rupture), and bowel ischemia [12,15]. The conditions in which complications occur during REBOA implementation are: 1) the physical damage inflicted on the accessing vessel (femoral artery or iliac vessels); and 2) ischemia and inflammation caused by blockage of downstream blood flow [15,16]. Vessels can be injured by the catheter itself or by overinflation of the REBOA balloon. Sadeghi et al. [16] reported that REBOA could cause severe systemic and intra-abdominal metabolic disturbances, organ damage, and inflammatory activation at 30 minutes of occlusion in a non-hemorrhagic porcine model.
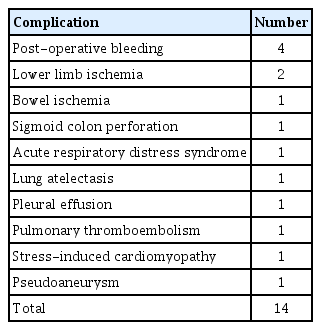
Description of complication
In this study, we attempted to identify the variables that affect the occurrence of complications (Fig. 2). In the LRA model, the occurrence of the complication is the dependent variable, and male sex and total occlusion have a statistically significant effect. However, this result is different from what we hypothesized. Males tend to have a higher risk of complications than females. This may have resulted from a bias that may have occurred during collection of data or due to the small amount of data (total number of patients was 54). In other studies, there is no evidence that males have a higher risk of occurrence of complications [13,15,17]. The judgment of this phenomenon should be withheld until more data is accumulated. The total occlusion of the REBOA balloon has a protective effect on complications than intermittent or partial occlusion. Usually, total occlusion is known to have a higher ischemic burden than partial occlusion [18]. The current guideline for REBOA recommends that total occlusion time in Zone 1 does not exceed 30-45 minutes [19]. However, there were three patients with ischemic complications in this study who received partial or intermittent occlusive REBOA, two of which were in Zone 3 and the other was in Zone 1. These ischemic complications occurred in a relatively early period of this study. It seems to be the complication caused by the patient’s condition or procedural immaturity, rather than problems associated with the type of REBOA. There was only one case in which the complication occurred in total occlusion. This result needs to be analyzed by considering the time that has been occluded rather than the REBOA type, and follow-up studies with data on the proficiency of REBOA and how to implement REBOA is also needed.
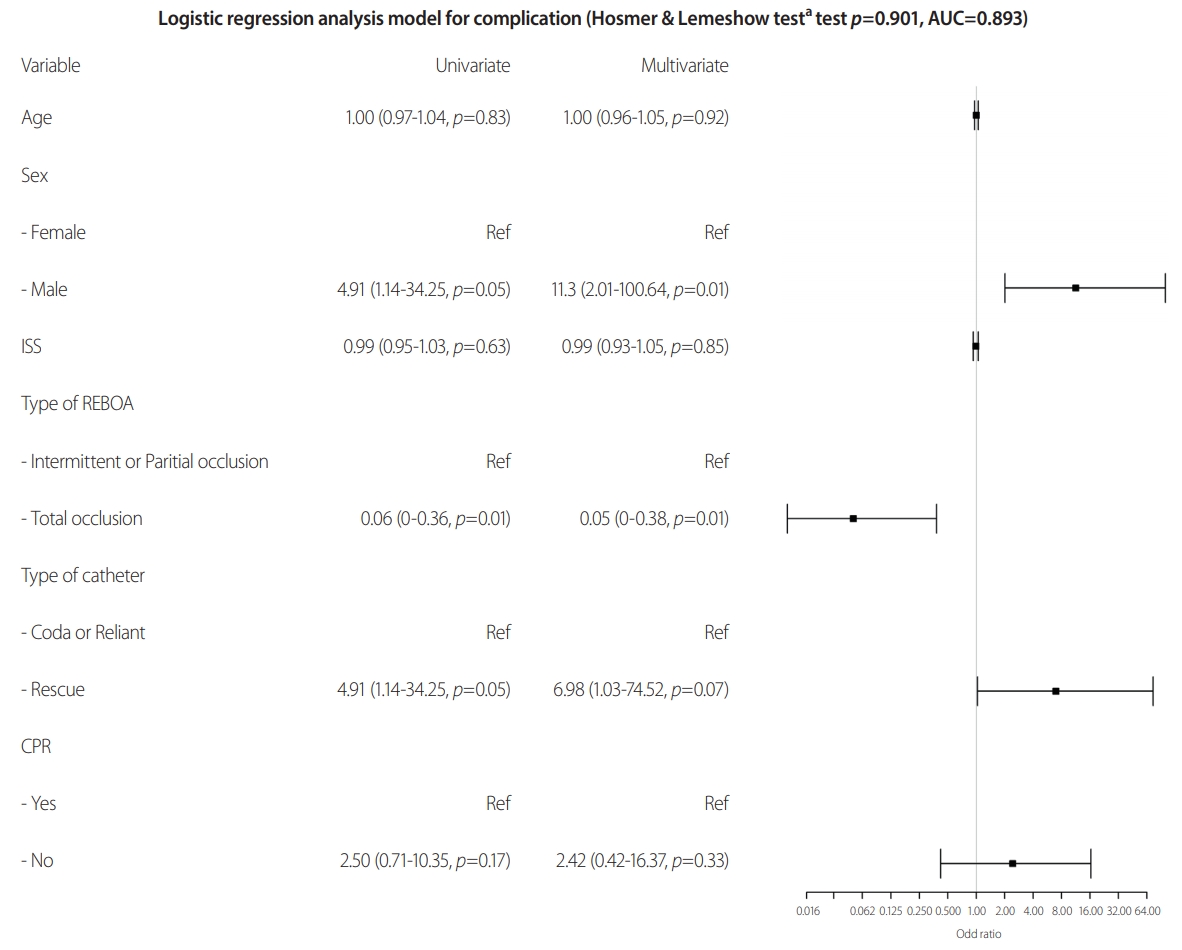
A logistic regression analysis model that the occurrence of the complication is the dependent variable. AUC: area under the receiver operating characteristic curve, ISS: injury severity score, REBOA: resuscitative endovascular balloon occlusion of the aorta, CPR: cardiopulmonary resuscitation. aHosmer and Lemeshow goodness of fit test.
The type of REBOA catheter is not statistically significant for the LRA model for complications. However, considering the 95% CI of this variable, Rescue catheters may have a dangerous effect on the occurrence of complications. The Rescue catheter is a 7 Fr catheter that reduces access-related complications and is safer than the previously used thick catheter [9,20,21]. Therefore, it cannot be concluded that the Rescue catheter has a dangerous effect on the occurrence of complications. During the study period, the Rescue catheter was used relatively later and had the largest number. Therefore, this result should be analyzed considering the time and frequency of use. Accordingly, it seems that this phenomenon is the result of insufficient proficiency in the overall REBOA procedure.
In the LRA model for death, we could not find any statistically significant variables except whether CPR was performed (Fig. 3). It should be considered that CPR itself is a powerful predictor of death, and REBOA is being implemented to buy time for the next treatment in patients with a high risk of death [9,22,23]. Therefore, further research with more accumulated data is necessary.
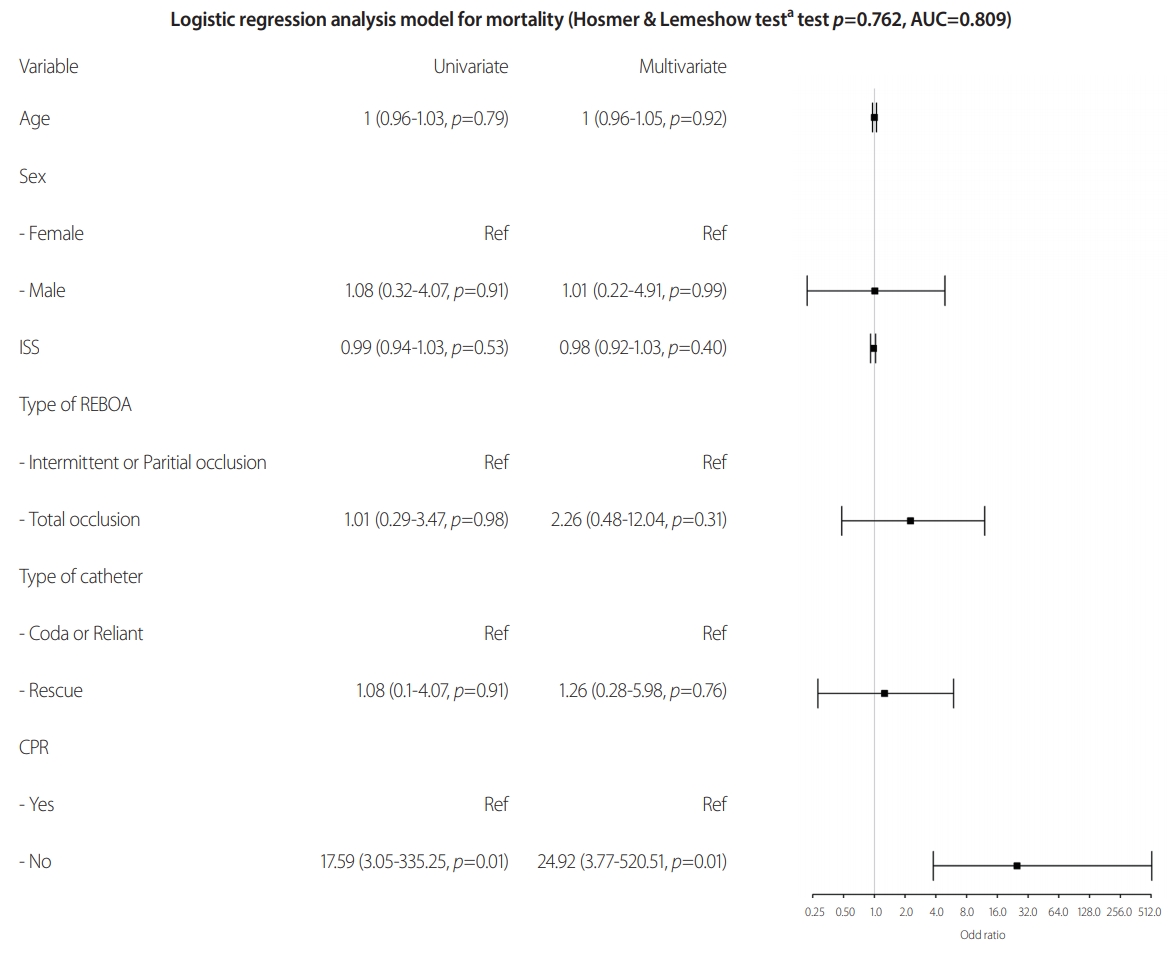
A logistic regression analysis model that mortality is a dependent variable. AUC: area under the receiver operating characteristic curve, ISS: injury severity score, REBOA: resuscitative endovascular balloon occlusion of the aorta, CPR: cardiopulmonary resuscitation. aHosmer and Lemeshow goodness of fit test.
CONCLUSION
REBOA is a technique that can improve hemodynamic stability in patients with life-threatening hemorrhagic shock. It seems that it can replace ERT in selective cases, but exact indications and protocols for REBOA have not been established. This study was conducted in the early stages of REBOA implementation in the Republic of Korea and showed conflicting results from studies conducted by multiple institutions. Therefore, additional research with more accumulated data is needed. Establishing appropriate protocols for REBOA and training for physicians is necessary.
Acknowledgements
We would like to thank Editage (www.editage.co.kr) for English language editing.