Postoperative infection after cranioplasty in traumatic brain injury: a single center experience
Article information

Abstract
Purpose
To determine the incidence and risk factors of postoperative infection after cranioplasty in patients with traumatic brain injury (TBI).
Methods
Data of 289 adult patients who underwent cranioplasty after TBI at a single regional trauma center between year 2018 and 2021 were reviewed retrospectively. Patient characteristics and various procedural variables, such as interval between craniectomy and cranioplasty, estimated blood loss, laterality and materials of the bone flap, and duration and classification of perioperative antibiotics usage were analyzed.
Results
Postoperative infection occurred in 17 patients (5.9%). Onset time of infectious symptom ranged from 9 days to 174 days (median, 24 days) after cranioplasty. The most common cultured organism was Staphylococcus aureus (47.1%), followed by Klebsiella pneumoniae (17.6%) and Enterococcus faecalis (17.6%). Patients with postoperative infection were more likely to have diabetes (odds ratio [OR], 6.96; 95% confidence interval [CI], 1.92–25.21; P=0.003), lower body mass index (OR, 0.81; 95% CI, 0.66–0.98; P=0.029), and shorter duration of perioperative antibiotics (OR, 0.83; 95% CI, 0.71–0.98; P=0.026).
Conclusions
For TBI patients with diabetes, poor nutritional status should be managed cautiously for increased risk of infection after cranioplasty. Further studies and discussions are needed to determine an appropriate antibiotics protocol in cranioplasty.
INTRODUCTION
Decompressive craniectomy is a widely used neurosurgical procedure to control increased intracranial pressure in multiple conditions including traumatic brain injury (TBI), stroke, and intracranial hemorrhage. When initial stage of hemorrhage and edema is over, cranioplasty is generally considered. Recent studies suggest that cranioplasty not only has protective and cosmetic benefit, but also is associated with functional neurological recovery [1,2].
However, cranioplasties can have serious complications including infection, seizures, bone resorption, and delayed hydrocephalus [3] with an overall complication rate reported as high as 40% [4]. Among these complications, postoperative infection is one of the most important complications because it can lead to serious conditions including empyema and meningitis, that require a long period of intravenous antibiotics treatment and possibly multiple surgeries.
Several studies have identified factors associated with infection after cranioplasty [3–6], mostly with heterogenous etiology and autologous bone graft. However, despite the recent development and increased usage of new graft materials, few attempts have been made to investigate infection risk of these newer material. Furthermore, lack of dedicated study in TBI population on this topic has not been addressed. In this study, authors provide comprehensive evaluation of incidence and risk factors of postoperative infection after cranioplasty in patients with TBI. This updated study might provide implications to achieve better care for TBI patients.
METHODS
Ethical statements
This study was approved by the Institutional Review Board of Pusan National University Hospital (No. 2207-023-117). Informed consent was waived due to the study’s retrospective nature.
Data collection and definition
Data of adult patients who underwent a cranioplasty at a single regional trauma center between year 2018 and 2021 were reviewed retrospectively. After excluding patients who underwent decompressive craniectomy for nontraumatic cause such as ischemic stroke, a total of 289 patients were enrolled. Their medical records were reviewed for information including age, sex, history of smoking, body mass index (BMI), Injury Severity Score at the time of initial trauma, American Society of Anesthesiologists physical status classification and modified Rankin Scale at the time of the cranioplasty. Procedural variables such as interval between craniectomy and cranioplasty, operational duration of cranioplasty surgery, estimated blood loss, laterality and materials of the bone flap, and duration and classification of perioperative antibiotics usage were also collected. Postoperative infection was defined as any case with one of the following presentations up to a year after cranioplasty as per Centers for Disease Control and Prevention definition of surgical site infection: purulent discharge, wound dehiscence, formation of abscess, or empyema with or without systemic inflammatory symptoms [7]. Degree of surgical site infections are usually classified as superficial incisional, deep incisional, and organ/space [7,8]. However, superficial incisional and deep incisional surgical site infections were often not clearly distinguishable by medical records and images. Therefore, infections with abscess, encephalitis, or meningitis were classified as organ/space infections and the rest were classified as incisional infections in this study.
Surgical technique
All cranioplasty were performed by five individual board-certified neurosurgeons with more than 2 years of experience as a neurotrauma surgeon in a standardized fashion. Surgical site was prepared in the usual manner. Previous incisions were reopened and dissected. Dural defects were repaired and sealed with collagen sponge (TachoSil; Takeda Austria, Linz, Austria). Cryopreserved autologous bone flaps were considered primarily in most cases. However, if the quality of bone flap was inadequate, various artificial grafts were considered based on surgeon’s and patient’s preference. Each implant, including cryopreserved autologous bone, polymethyl methacrylate, polyether ether ketone, or titanium mesh implant, was sterilized using ethylene oxide gas and irrigated vigorously with normal saline before implantation. All graft were fixated with miniplates and two subgaleal drains were placed before closure of the surgical wound.
Prophylactic antibiotics were administered within 1 hour of skin incision. However, the choice of antibiotics and the duration of usage varied greatly per surgeon’s preference and the clinical scenario. If prophylactic antibiotics were used continuously more than 2 weeks for the treatment of various infections such as pneumonia and phlebitis, they were still counted as perioperative antibiotics for the purpose of this study.
Statistical method
After collection, data were divided into an infection group and a non-infection group. Independent t-test or Wilcoxon rank-sum test for continuous variable and chi-square test or Fisher exact test for categorical variable were used for initial analysis. Multivariate logistic regression was also performed to evaluate statistical correlation. Odds ratio (OR) and 95% confidence interval (CI) were calculated when applicable. Two tailed P-values of less than 0.05 were considered to indicate statistical significance. All statistical analyses were conducted using R ver. 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
A total of 289 patients underwent cranioplasty during the 4-year period (2018 to 2021), including 219 male patients (76.3%). The mean age of patients was 51.6 years (Table 1). A total of 17 patients (5.9%) had postoperative infection. Onset time of infectious symptom ranged from 9 to 174 days (median, 24 days) after cranioplasty (Table 2). Thirteen of 17 patients (76.5%) with surgical infection had organ/space infection such as epidural/subdural abscess and meningitis. The most commonly cultured organism was Staphylococcus aureus (47.1%), followed by Klebsiella pneumoniae (17.6%) and Enterococcus faecalis (17.6%) (Table 3).
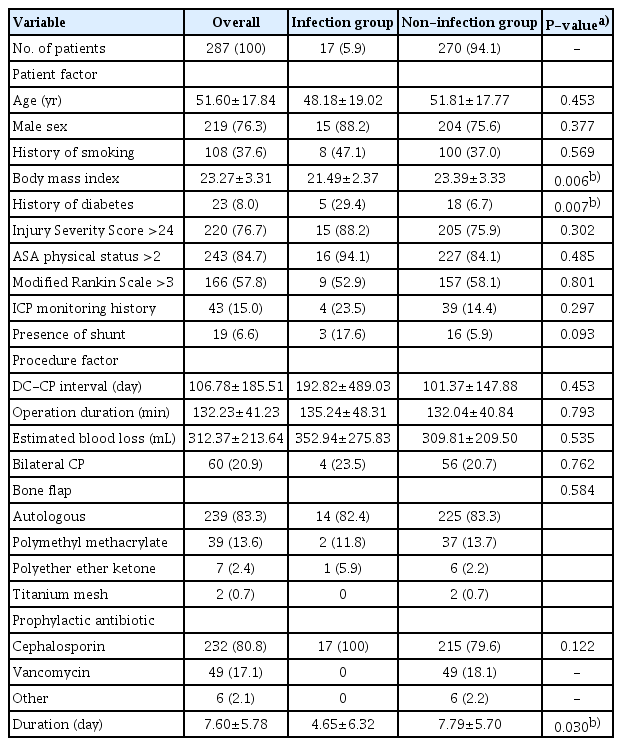
Summary of patient characteristic and possible risk factors

Multivariate logistic regression analysis
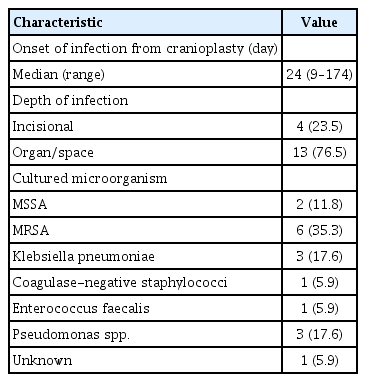
Characteristics of postoperative infection cases (n=17)
In initial statistical analysis between the infection group and the non-infection group, variables showing statistically significant difference included BMI (P=0.006), diabetes (P=0.007), and duration of perioperative antibiotics usage (P=0.030). In multivariate logistic regression analyses, patients in the infection group were more likely to have diabetes (OR, 6.96; 95% CI, 1.92–24.21; P=0.003) and lower BMI (OR, 0.81; 95% CI, 0.66–0.98; P=0.029) (Table 2). Other patient factors including age, sex, history of smoking, Injury Severity Score, American Society of Anesthesiologists physical status, modified Rankin Scale, history of continuous intracranial pressure monitoring, and presence of shunt device were not associated with postoperative infection. Procedural factors did not show any significant associations with postoperative infection either. However, a shorter duration of perioperative antibiotics usage was associated with an increased infection risk (OR, 0.83; 95% CI, 0.71–0.98; P=0.026). We did not observe any significant difference in infection rates between individual surgeons (P=0.69) (Table 4).
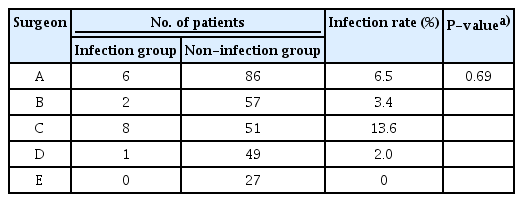
Infection rate of individual surgeons
DISCUSSION
Diabetes has been associated with various postoperative morbidity, including postoperative infection after cranioplasty [3,4,6]. In this study, we also found a strong correlation between diabetes and infection. The only other patient factor that showed a statistically significant association with infection in our study was BMI. In the designing stage of this study, we suspected that obesity would be associated with infection. However, we observed a trend of association between higher BMI and decreased risk of postoperative infection. Considering that many patients with TBI are bed ridden, their nutritional status might be related to the incidence of infection. Although a few studies have discussed the correlation between malnutrition and surgical infection [9,10], further investigation is needed on this topic. Previous surgical procedures such as history of continuous monitoring and presence of shunt device were presumed to increase risk of infection. However, they did not affect infection incidence significantly in our study.
With recent advancement in technology, more and more patients are getting three-dimensional printed polyether ether ketone grafts which offer better cosmetic outcome and shorter operation time than traditional free hand molded polymethyl methacrylate grafts. Therefore, the authors included various types of cranioplasty materials in this study, different from previous studies that focused on autologous graft and first time cranioplasty. However, we did not observe any significant difference in the incidence of postoperative infection depending on the graft material. Punchak et al. [11] have published a meta-analysis on the safety of polymethyl methacrylate graft without reaching conclusion on the implant infection risk due to the lack of data. Other variables such as timing and duration of the cranioplasty, as well as estimated blood loss did not affect the infection risk either.
There is no clear guideline on perioperative antibiotics usage in a cranioplasty surgery specifically. However, the 2017 Centers for Disease Control and Prevention guideline strongly recommends against repeated use of prophylactic antibiotics usage in clean or clean-contaminated procedure [12]. Surgical Infection Society guideline also recommends single-dose antibiotics without a clearly recommended choice of agent [13]. However, in clinical practice, these recommendations are not always followed strictly. Single-dose antibiotics administration was used only in 39 cases (13.5%) in our study (Fig. 1). Often, cranioplasty is considered as “an implantation surgery” associated with high infection rate and biofilm formation. Furthermore, because many patients were critically ill and exposed to antibiotics resistant microorganisms, some studies even suggest routine use of vancomycin [14] or when the patient carries methicillin-resistant S. aureus on a scalp swap [15]. In our study, we observed that a shorter duration of perioperative antibiotics associated with a higher infection risk. Though results of this study are insufficient to conclude optimal protocol on antibiotics usage in cranioplasty, surgeons might need to consider extended duration of perioperative antibiotics, especially in high infection risk patients.
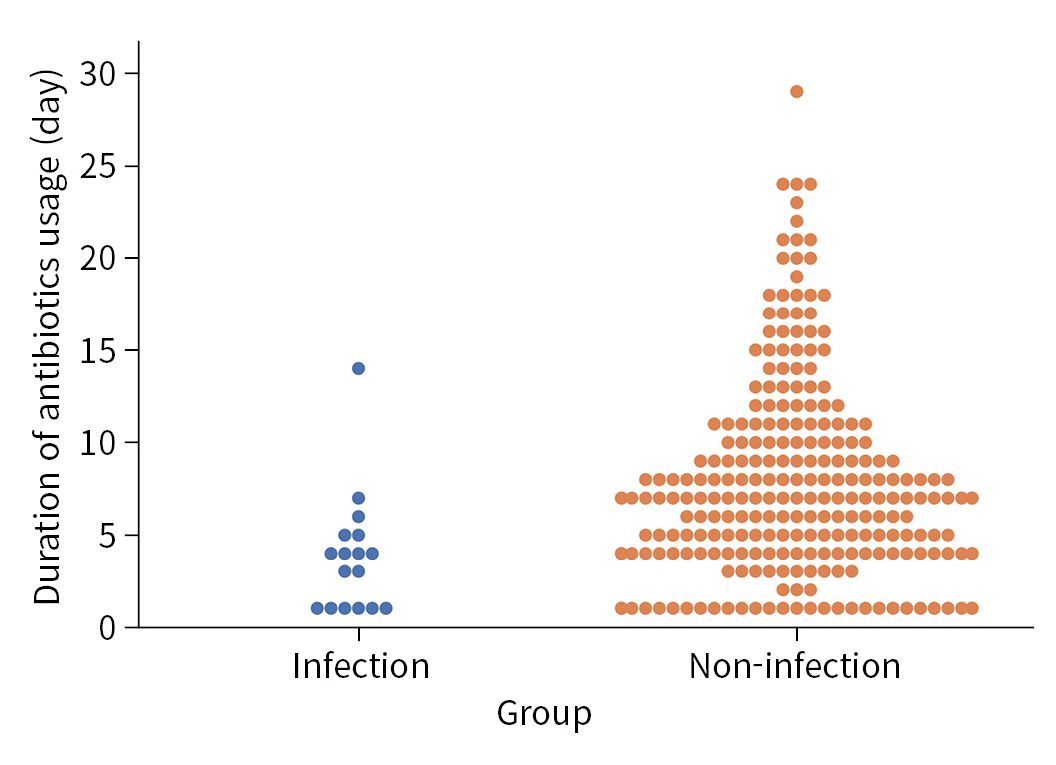
Duration of perioperative antibiotics usage.
This study has a few limitations. First, this was a retrospective, nonrandomized single center study with a relatively small number of patients, especially infection group (17 patients). Second, due to the goal of this study to search for risk factors, data were more heterogenous than those of previous studies that usually focus on first time cranioplasty with autologous bone graft. Factors such as skin flora, size of craniectomy, damage of skin in the initial trauma should be included in future studies. Further randomized prospective studies with larger sample sizes are also needed.
Despite the limitations, this study demonstrates that diabetes, lower BMI, and shorter duration of perioperative antibiotics are correlated with a higher chance of postoperative infection after cranioplasty in patients with TBI. Since postoperative infections have major negative effect on the course of the treatment of TBI, surgeons should pay attention to modifiable factors when performing cranioplasty. Tighter blood sugar control with sufficient nutrition and adequate use of antibiotics might help reduce the risk of postoperative infections.
Notes
Ethical statements
This study was approved by the Institutional Review Board of Pusan National University Hospital (No. 2207-023-117). Informed consent was waived due to the study’s retrospective nature.
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
This work was supported by a clinical research grant from Pusan National University Hospital in 2022.
Author contributions
Conceptualization: SY; Data curation: MH, HJC, BCK; Formal analysis: JHL; Funding acquisition: BCK; Methodology: HJC, BCK; Project administration: JHL, HJC, SY; Visualization: JHL; Writing–original draft: MH; Writing–review & editing: HJC, BCK, SY.
All authors read and approved the final manuscript.