Articles
- Page Path
- HOME > J Trauma Inj > Volume 36(1); 2023 > Article
-
Case Report
Azygos and right superior intercostal vein injury secondary to blunt trauma: a case report -
Nima Yaftian, MD
 , Benjamin Dunne, MD, Phillip Antippa, MBBS
, Benjamin Dunne, MD, Phillip Antippa, MBBS -
Journal of Trauma and Injury 2023;36(1):53-55.
DOI: https://doi.org/10.20408/jti.2022.0001
Published online: July 21, 2022
- 1,677 Views
- 42 Download
Department of Cardiothoracic Surgery, Royal Melbourne Hospital, Parkville, Australia
- Correspondence to Nima Yaftian, MD Department of Cardiothoracic Surgery, Royal Melbourne Hospital, 300 Grattan Street, Parkville, Victoria 3050, Australia Tel: +61-3-9342-7000 Email: nimayaftian@gmail.com
Copyright © 2023 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- Azygos vein injuries are rare consequences of blunt trauma. When there is high drainage output from a right-sided intercostal catheter, an azygos injury must be considered in the differential diagnosis. We report the case of a 38-year-old male patient involved in a fall from a height during a motorcycle accident. Computed tomography demonstrated a large right-sided hemothorax and left-sided pneumothorax. The patient was transferred to the operating theatre and underwent a clamshell thoracotomy. A laceration in the azygos vein at the confluence of the arch of the azygos and the right superior intercostal vein was identified. Bleeding was controlled at the trifurcation. The patient survived and was discharged home on postoperative day 15.
- Injuries to the azygos vein following blunt trauma are rare and associated with significant morbidity and mortality. We describe the case of a patient who presented with a laceration of the azygos and superior intercostal veins secondary to a motorbike accident.
INTRODUCTION
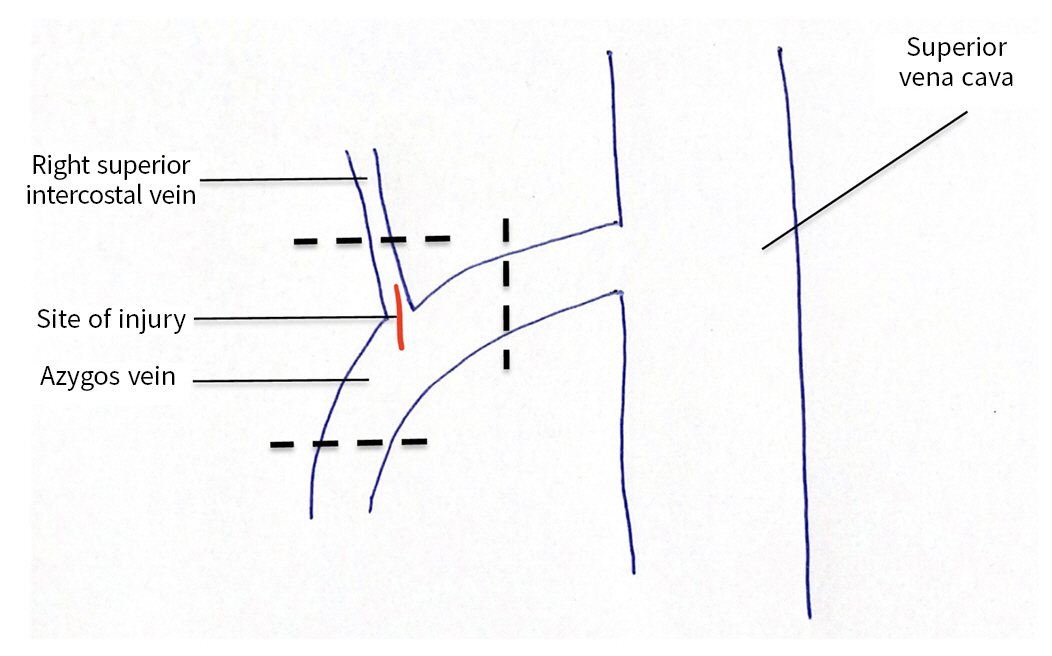
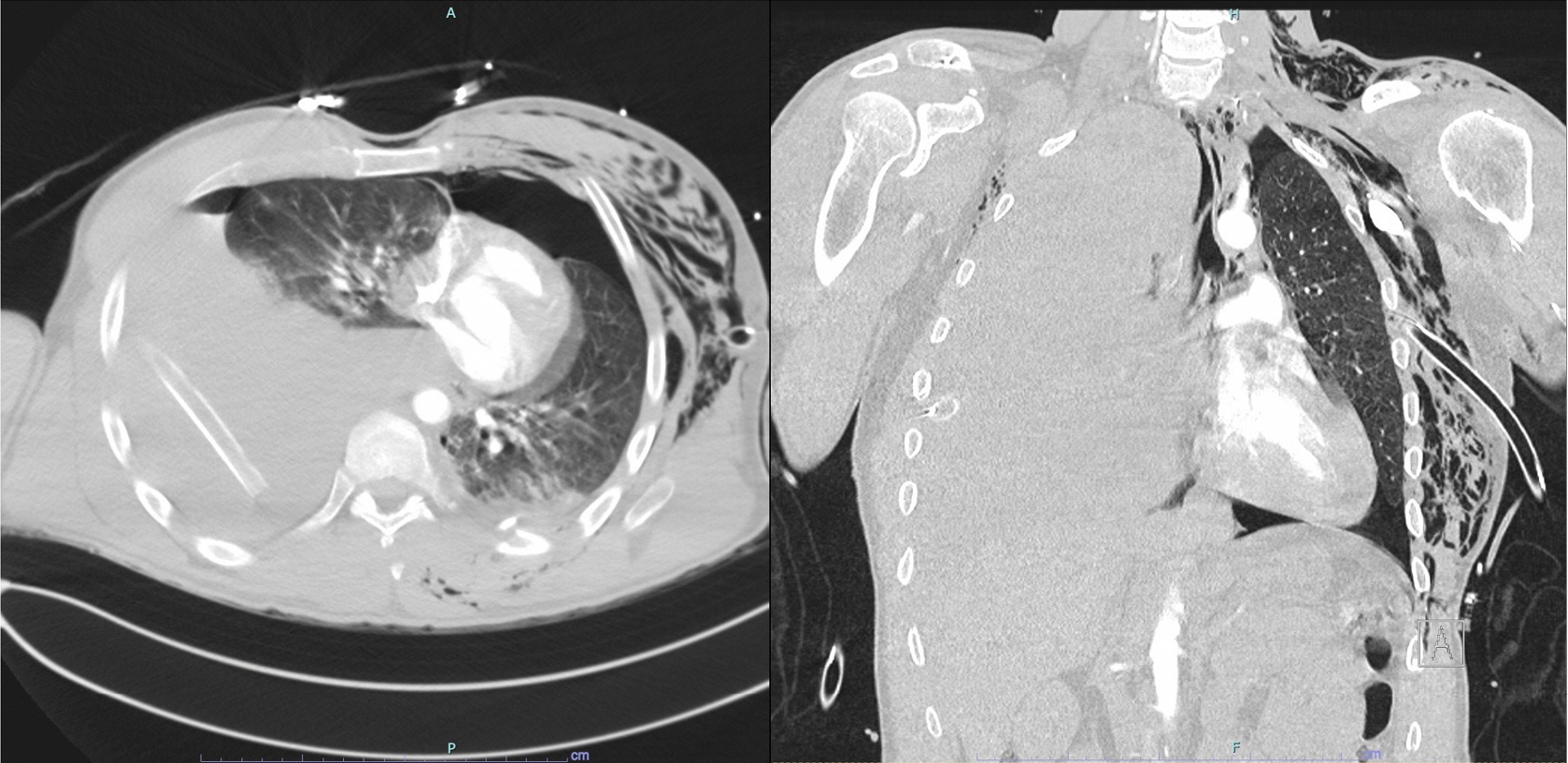
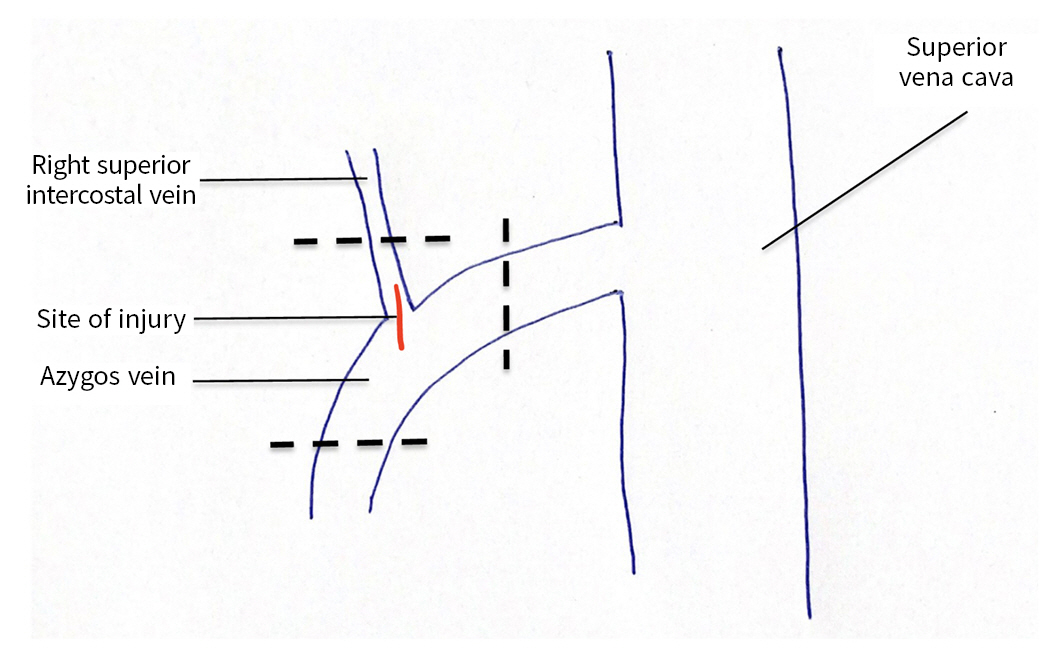
- A 38-year-old male patient presented with hypotension and tachycardia following an unsuccessful attempted 8-m jump on an off-road motorbike. An endotracheal tube was inserted upon presentation to the emergency department and the patient was fluid-resuscitated with a massive exsanguination pack, which consisted of 4 units of red blood cells, 4 units of fresh frozen plasma, and 4 units of platelets. The patient was found to have a large left-sided pneumothorax and large right-sided hemothorax with white-out on the chest radiograph performed on presentation. Bilateral intercostal catheters (ICCs) were inserted. The right ICC had 1,300 mL of blood upon insertion with a further 200 mL over the next hour. The left ICC had 300 mL of output and the patient’s left lung was partially reexpanded. Thoracic surgery was consulted regarding the ongoing high-volume drain tube output from the right-sided ICC. The patient was reviewed by thoracic surgery in the emergency department. Given the uncertainty regarding the etiology of the injury and the patient’s transient improvement in hemodynamic response to fluid resuscitation a decision was made to perform a computed tomography scan of the patient’s chest. This was performed in the brief period of hemodynamic stability following fluid resuscitation. The computed tomography scan showed a persistent large-volume right-sided hemothorax and a persistent left-sided pneumothorax (Fig. 1). The patient was taken to the operating theatre and a clamshell thoracotomy was performed. The pericardium was opened and a sling was placed around the right main pulmonary artery and superior vena cava intrapericardially. The chest was explored and a laceration was identified at the confluence of the azygos vein and the right superior intercostal vein that extended down both veins. The azygos vein was divided and staple-ligated distal to the confluence with the superior vena cava and inferior to its confluence with the superior intercostal vein using an Echelon Flex powered vascular stapler (Johnson & Johnson, New Brunswick, NJ, USA). The superior intercostal vein was divided and staple-ligated superior to its confluence with the azygos vein (Fig. 2).
- Other injuries that required surgery during the admission included a displaced and a comminuted fracture of the left ileum and L4 left inferior articular facet joint. Other injuries that did not require intervention were nondisplaced fractures of the left ribs 1–10 posteriorly and anterolaterally, a T3 transverse process fracture, and a T7 spinous process fracture. The patient was extubated on postoperative day 5 and transferred to the ward. He was discharged home on day 15 postoperatively. The patient was well when seen in clinic 1 month postdischarge.
- Informed consent was obtained from the patient in line with the Royal Melbourne Hospital Research Governance Unit case report policy. A literature review on traumatic azygos injuries was conducted.
CASE REPORT
- There are a number of reports in the literature regarding azygos vein injuries secondary to trauma. These are significant injuries, and a literature review showed that they were associated with a 35% mortality rate [1]. Often, the diagnosis is only made at the time of autopsy. Some patients can be taken to the operating room without a definitive diagnosis for high right-sided ICC output or hemodynamic instability and right-sided chest trauma. In many cases the diagnosis of azygos vein injury is made following computed tomography imaging [1,2]. If a diagnosis of azygos vein injury is made prior to transfer to the operating room, a right-sided thoracotomy would allow appropriate visualization and access to the azygos vein to facilitate control of hemorrhage and repair of injury [2]. However, when a definitive diagnosis has not been made prior to surgery and the location of the injury is unclear, then the decision regarding surgical access becomes more pertinent. In this case, there was concern about potential left-sided injuries given the presence of blood in the left chest and residual pneumothorax. A diagnosis of azygos vein injury was only made intraoperatively. Following a brief initial discussion, a decision was made to perform a clamshell thoracotomy with the rationale that with two senior surgeons present in the operating room, it would provide the fastest access to both the right and chest. This decision was made based on the surgeons’ experience with the management of thoracic trauma and the previously published literature [3]. This was thought at the time to be safer and more time-efficient than extending both a right-sided and left-sided thoracotomy. Median sternotomy has been used successfully for access to azygos vein injuries [4]. However, it was the operating surgeons’ opinion that median sternotomy would not have allowed timely visualization of the hilar and posterior mediastinal structures. In retrospect, the authors felt that given the losses, the extent of the injury to the vein, and hemodynamic instability, performing a sternotomy would have added a significant time delay to the identification and control of the injury.
- There are multiple potential mechanisms of azygos vein injuries in blunt trauma. These include sheer force injuries at the confluence of the fixed azygos vein and mobile azygos arch, a rapid rise in venous pressure from cardiac compression, and direct injury from fractured vertebrae [2,4]. In this case, given the location of the rupture, the most likely mechanism was a shear force injury, as the location of the injury was at the confluence of the azygos vein and azygos arch [4].
- Blunt traumatic injuries of the azygos vein are rare and fatal if not diagnosed and treated promptly. Aggressive fluid resuscitation and early thoracic surgical intervention are crucial for survival. In the appropriate circumstances, a clamshell thoracotomy provides excellent access and exposure to identify unknown thoracic injuries.
DISCUSSION
-
Ethical statements
Informed consent was obtained from the patient in line with the Royal Melbourne Hospital Research Governance Unit case report policy.
-
Conflicts of interest
The authors have no conflicts of interest to declare.
-
Funding
None.
-
Author contributions
Conceptualization: all authors; Methodology: NY; Visualization: NY; Writing–original draft: NY; Writing–review & editing: BD, PA. All authors read and approved the final manuscript.
ARTICLE INFORMATION
- 1. Nguyen LL, Gates JD. Simultaneous azygous vein and aortic injury from blunt trauma: case report and review of the literature. J Trauma 2006;61:444–6. ArticlePubMed
- 2. Endara SA, Davalos GA, Nunez MF, Manzano JE. Azygous vein laceration secondary to blunt thoraco-abdominal trauma. Interact Cardiovasc Thorac Surg 2010;11:342–4. ArticlePubMed
- 3. Simms ER, Flaris AN, Franchino X, Thomas MS, Caillot JL, Voiglio EJ. Bilateral anterior thoracotomy (clamshell incision) is the ideal emergency thoracotomy incision: an anatomic study. World J Surg 2013;37:1277–85. ArticlePubMedPDF
- 4. Drac P, Manak P, Klein J, Kral V. Azygos vein injury in blunt chest trauma. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 2007;151:347–8. ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite