
Articles
- Page Path
- HOME > J Trauma Inj > Volume 36(4); 2023 > Article
-
Case Report
A method of bedside urethrography before catheterization in pelvic trauma in Korea: a case report -
Hojun Lee, MD1
 , Sung Yub Jeong, MD2, Kun Hwang, MD2,3
, Sung Yub Jeong, MD2, Kun Hwang, MD2,3 -
Journal of Trauma and Injury 2023;36(4):451-453.
DOI: https://doi.org/10.20408/jti.2023.0047
Published online: December 20, 2023
- 259 Views
- 7 Download
1Department of General Surgery, Armed Forces Capital Hospital, Seongnam, Korea
2Department of Plastic Surgery, Armed Forces Capital Hospital, Seongnam, Korea
3Ewha Medical Academy, Ewha Womans University Medical Center, Seoul, Korea
- Correspondence to Kun Hwang, MD Department of Plastic Surgery, Armed Forces Capital Hospital, 81 Saemaeul-ro 177 beon-gil, Bundang-gu, Seongnam 13574, Korea Tel: +82-31-725-6406, Email: jokerhg@naver.com
Copyright © 2023 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
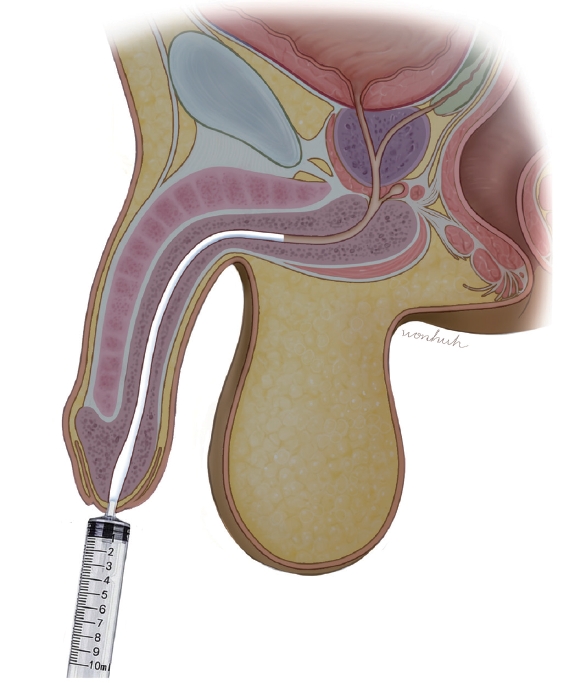
- We introduce a convenient method of urethrography before catheterization for patients with pelvic trauma that can be used in a resuscitation area. A 10-mL syringe without a needle was used. X-ray contrast medium (Iohexol, 300 mg I/mL) was administered through the urethral orifice using a 10-mL syringe without needle and a simple pelvic anteroposterior film was taken (70 kilovolt [peak], 50 mAs). A 36-year-old soldier with a saddle injury from a gun barrel was taken to a trauma center. He had a pelvic fracture and complained of hematuria. Bedside urethrography above described was performed. The anterior urethra showed nonspecific findings, but dye leaked from the posterior urethra. Bedside Foley catheter insertion was attempted, but the catheter could not be advanced past the membranous urethra. Thereafter, suprapubic catheterization was performed. On the day of the injury, iliac artery embolization was carried out. The dislocated sacroiliac joint was also treated using open reduction and internal fixation. On hospital day 7, guidewire Foley insertion was performed. This bedside urethrography technique is simple and useful for pelvic fractures in which urethral injury is suspected.
- Urethral injury is a common complication of pelvic trauma, and significant long-term morbidity can occur if it is undiagnosed. Segments of the urethra that are near the pubic rami and the puboprostatic ligaments are particularly vulnerable. Although computed tomography is commonly used for the initial imaging evaluation of patients with polytrauma, urethral injury is better assessed and classified using urethrography. Complete urethral imaging is especially important at presentation because the insertion of a transurethral bladder catheter may exacerbate an existing injury (e.g., by causing a partial urethral tear to become a complete transection). However, urethrography after pelvic trauma may be difficult because the patient is immobile or a surgical fixation device is present [1].
- We introduce a convenient method of urethrography before catheterization for patients with pelvic trauma that can be used in a resuscitation area. A 10-mL syringe without a needle was used. X-ray contrast medium (Iohexol, 300 mg I/mL) was administered through the urethral orifice using a 10-mL syringe without needle (Fig. 1) and a simple pelvic anteroposterior (AP) film was taken (70 kilovolt [peak], 50 mAs).
INTRODUCTION
- A 36-year-old soldier with a saddle injury from a gun barrel was taken to the Armed Forces Trauma Center (Seongnam, Korea). He had a pelvic fracture and complained of hematuria.
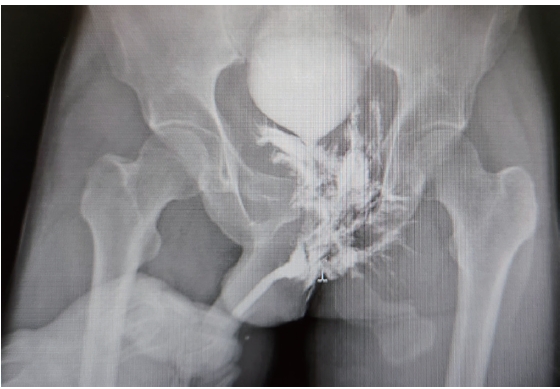
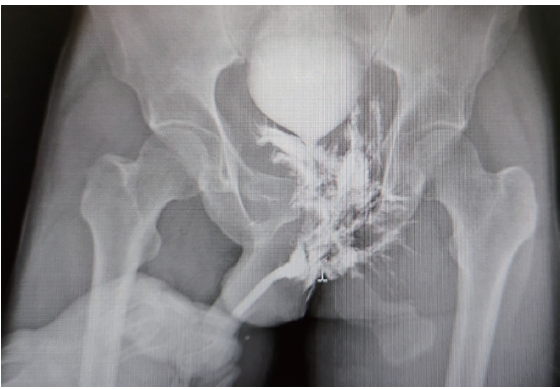
- Bedside urethrography was performed. X-ray contrast medium was administered through the urethral orifice using a 10-mL syringe without a needle, and a simple pelvic AP film was taken. The anterior urethra showed nonspecific findings, but dye leaked from the posterior urethra (Fig. 2). Bedside Foley catheter insertion was attempted, but the catheter could not be advanced past the membranous urethra. Thereafter, suprapubic catheterization was performed.
- On the day of the injury, iliac artery embolization was carried out. The dislocated sacroiliac joint was also treated using open reduction and internal fixation. On hospital day 7, guidewire Foley insertion was performed.
- Ethics statement
- This study adhered to the principles outlined in the Declaration of Helsinki. Written informed consent for publication of the research details and clinical images was obtained from the patient.
CASE REPORT
- Urethral injury is a common complication of pelvic trauma, occurring in as many as 24% of adults with pelvic fractures [2]. The most common site of these injuries by far is the posterior urethra. These injuries occur in 3% to 25% of patients with pelvic fractures [3].
- The usage of a Foley catheter in ascending urethrography has several disadvantages: trauma to the urethra, inability to examine the anterior urethra, and slipping of the catheter out of the urethra during the examination, especially in cases of impassable urethral strictures [4]. Researchers have invented devices for retrograde urethrography; however, they were primarily suitable for prostatic calculi, calcification in the bladder, urethral calculi, or radio-opaque foreign bodies [4,5]. For male infants, a 5F or 8F end-hole polyethylene catheter was bound to the meatal orifice with a surgical tape during retrograde urethrography [6].
- However, the above instruments and techniques were not convenient for the examination of pelvic injuries, especially in the resuscitation theater. As described in the present paper, x-ray contrast medium was administered through the urethral orifice using a 10-mL syringe without a needle, and a simple pelvis AP film was taken.
- In our case, after the surgery, interventional radiologist recommended guidewire Foley insertion to prevent urethral stricture. Urologist preferred spontaneous urethral healing. Thereafter, guidewire Foley was inserted on the 7th hospital day.
- This bedside urethrography technique is simple and useful for pelvic fractures in which urethral injury is suspected.
DISCUSSION
-
Author contributions
Conceptualization: HL; Funding acquisition: KH; Investigation: SYL, KH; Methodology: SYL; Project administration: HL, KH; Supervision: SYL; Visualization: KH; Writing–original draft: HL, KH; Writing–review & editing: all authors. All authors read and approved the final manuscript.
-
Conflicts of interest
Kun Hwang is an Editorial Board member of the Journal of Trauma and Injury, but was not involved in the peer reviewer selection, evaluation, or decision process of this article. The authors have no other conflicts of interest to declare.
-
Funding
This study was supported by the Korean Military Medical Research Project funded by the ROK Ministry of National Defense (No. ROK-MND-2023-KMMRP-020).
-
Acknowledgments
The authors thank Hye Won Hu, MA (Department of Oral Biology, Yonsei University College of Dentistry, Seoul, Korea) for her illustration.
-
Data availability
Data sharing is not applicable as no new data were created or analyzed in this study.
ARTICLE INFORMATION
- 1. Ingram MD, Watson SG, Skippage PL, Patel U. Urethral injuries after pelvic trauma: evaluation with urethrography. Radiographics 2008;28:1631–43. ArticlePubMed
- 2. Koraitim MM. Pelvic fracture urethral injuries: evaluation of various methods of management. J Urol 1996;156:1288–91. ArticlePubMed
- 3. Patel U, Rickards D. Imaging and urodynamics of the lower urinary tract. Taylor & Francis; 2005.
- 4. Kwi NK. A simple instrument for ascending urethrography in males. Med J Malaya 1972;26:291–2.
- 5. Berna-Mestre JD Jr, Berna-Serna J. A perfected device for performing retrograde urethrography. Med Devices (Auckl) 2008;1:19–21. PubMedPMC
- 6. Lucaya J. A simple technique of retrograde urethrography in male infants. Radiology 1972;102:402. ArticlePubMed
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-

- Related articles
-
- One year of treating patients with open fractures of the lower extremity in a new military trauma center in Korea: a case series
- Massive traumatic abdominal wall hernia in pediatric multitrauma in Australia: a case report
- Spontaneous recanalization of complete urethral injury treated by suprapubic cystostomy alone after severe pelvic bone fracture in a young male in Korea: a case report
- Delayed bladder perforation due to screw loosening after pelvic ring injury surgery: a case report

